This topic contains a solution. Click here to go to the answer
|
|
|

 Using alert labels enables the medical staff to quickly identify important information such as ...
Using alert labels enables the medical staff to quickly identify important information such as ...
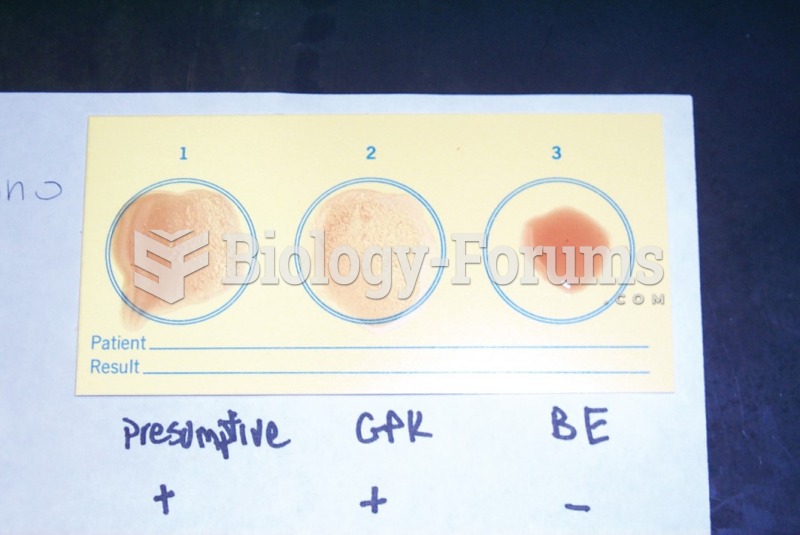 A Mono-Diff test in which the presumptive well contains the patient's serum mixed with ...
A Mono-Diff test in which the presumptive well contains the patient's serum mixed with ...
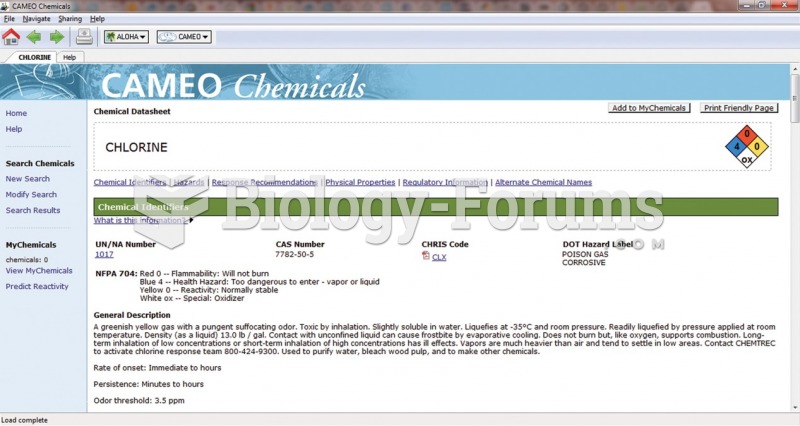 The CAMEO entry for chlorine. Useful information includes chemical and physical properties, personal ...
The CAMEO entry for chlorine. Useful information includes chemical and physical properties, personal ...
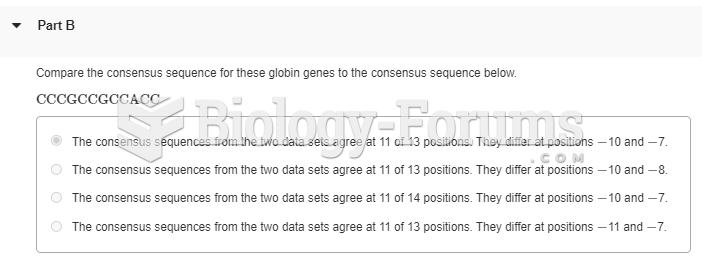 8.The following table contains DNA-sequence information compiled by Marilyn Kozak (1987). The ...
8.The following table contains DNA-sequence information compiled by Marilyn Kozak (1987). The ...
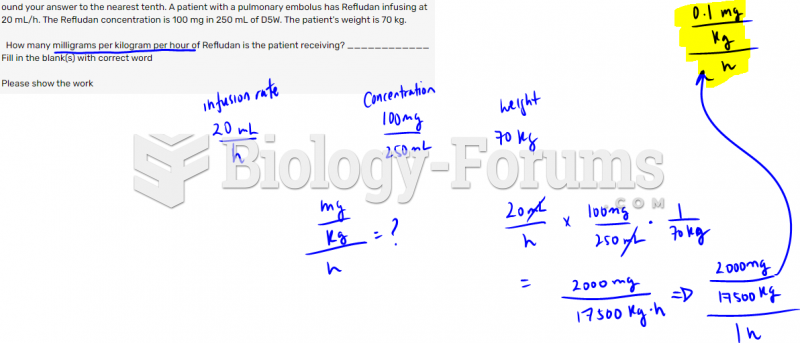 Round your answer to the nearest tenth. A patient with a pulmonary embolus has Refludan ...
Round your answer to the nearest tenth. A patient with a pulmonary embolus has Refludan ...