Answer to Question 1
B, C, D
The EHR streamlines many documentation steps, making written communication concise and standardized. Electronic access to the patient's health record increases confidentiality and security of information by using customized passwords for each healthcare professional to limit access to the records. Time for documentation is decreased as the nurse becomes more comfortable using electronic documentation. Medical errors are decreased owing to programmed alerts that are automatically displayed when a healthcare provider takes an action that could potentially be harmful to the client. The EHR facilitates communication of client care across the healthcare team because all of the information is in one place and multiple people can access it from different computers at the same time.
Answer to Question 2
C, D, E, F
Heparin, an anticoagulant, should be given to achieve one and a half to two times the normal clotting times and PTT. Because the findings of the laboratory values are four times the normal range and petechiae are present, this indicates a significant risk for bleeding. Therefore, the heparin should be held; the physician should be notified immediately. The nurse must document why the medication was not given and should assess for other significant findings. Omitted or delayed administration must be charted as soon as possible with an explanation for the delay or omission. The nurse will notify the provider but not give the medication. Heparin is given via a subcutaneous injection; however, because it is being held, it will not be administered or documented as given. Because the findings regarding the heparin and its use are abnormal, the nurse would not document normal findings.

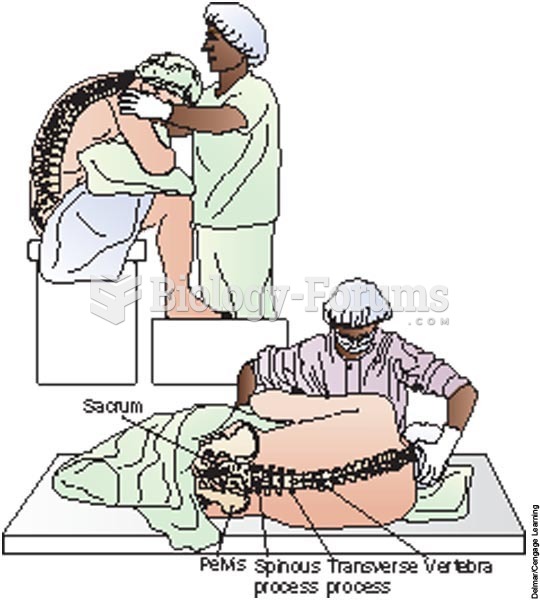 The surgical nurse assists the client into the correct position
The surgical nurse assists the client into the correct position
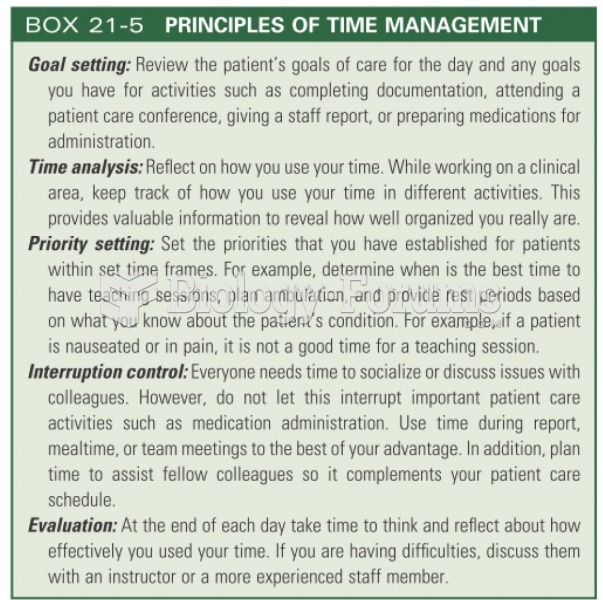 Principles of time management
Principles of time management
 Both individuals and organizations do impression management, trying to communicate messages about ...
Both individuals and organizations do impression management, trying to communicate messages about ...
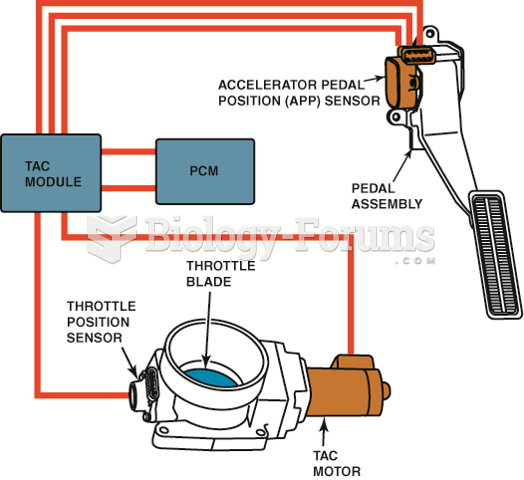 The throttle pedal is connected to the accelerator pedal position (APP) sensor. The electronic ...
The throttle pedal is connected to the accelerator pedal position (APP) sensor. The electronic ...
 Radioactive protection services record book and two badge-style dosimeters.
Radioactive protection services record book and two badge-style dosimeters.
 Management Information Systems: Managing the Digital Firm, 15th Edition
Management Information Systems: Managing the Digital Firm, 15th Edition