Answer to Question 1
The lab values that stand out as strong indicators of renal disease are BUN and creatinine. Several other lab values are supportive of renal disease in that they indicate conditions that usually accompany renal failure, i.e. all the labs that indicate anemia (MCV, Hgb, Hct), the elevated electrolytes (Na and K), the elevated P and uric acid, and the depressed Ca. In the urinalysis, the SG, +2 protein, and the pH all indicate possible renal failure.
Answer to Question 2
Renal disease and HTN can be associated in more than one way. Assume that a person has untreated HTN from some unknown cause. Longstanding elevated blood pressure can result in left ventricular hypertrophy. If it remains untreated, this can culminate in congestive heart failure. The increased blood pressure increases the incidence of atherosclerosis, which increases the blood pressure further2.
As the BP increases and left-sided heart failure progresses, blood flow to the kidneys decreases. Since the kidneys are dependent on the BP to force fluid through the glomerulus for filtration, the drop in BP in the kidneys causes them to set the renin - angiotensinogen cycle in motion. This raises the BP even higher and intensifies the situation. The GFR remains normal until late in the disease process. The kidneys begin to degenerate and this results in the filtration fraction increasing along with elevated protein in the urine.
Another approach to renal disease and HTN could be from the perspective that a malfunctioning kidney causes an increase in BP by the excretion of renin when the BP is normal, thus starting a cycle that continues to increase the BP as follows: renin angiotensinogen I angiotensinogen II increases BP causes atherosclerosis increases BP even more causes left sided heart failure decreases blood flow to the kidneys causes additional secretion of renin.

 (a) Feeding by bear on salmon results in large allochthonous inputs of nutrients into (b) the forest
(a) Feeding by bear on salmon results in large allochthonous inputs of nutrients into (b) the forest
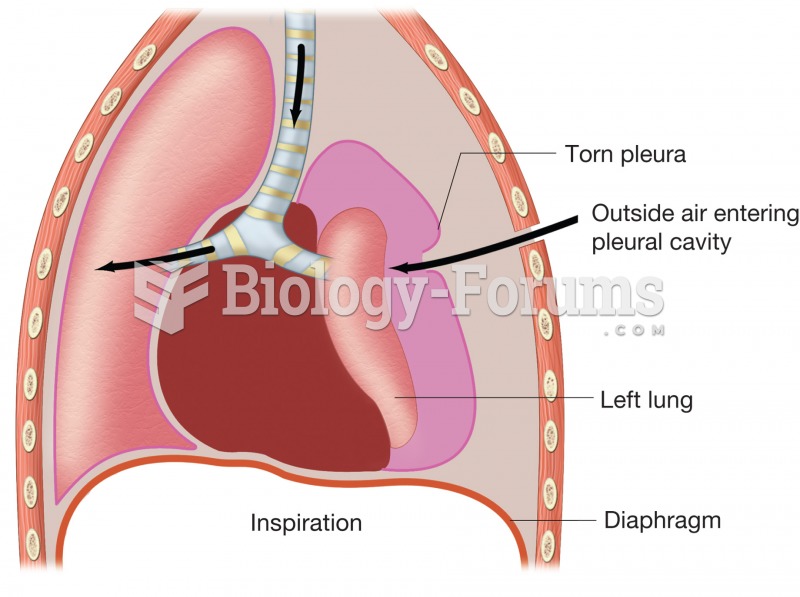 Pneumothorax. Figure illustrates how puncture of thoracic wall and tearing of pleural membrane allow
Pneumothorax. Figure illustrates how puncture of thoracic wall and tearing of pleural membrane allow
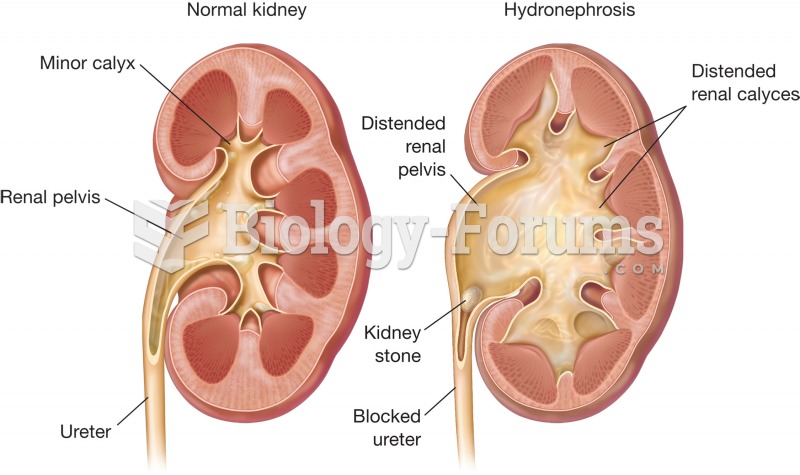 Hydronephrosis. Normal kidney (left) and kidney with hydronephrosis (right) are compared. Note the d
Hydronephrosis. Normal kidney (left) and kidney with hydronephrosis (right) are compared. Note the d
 Carrie Mae Weems, Untitled (Man Smoking/Malcolm X), from The Kitchen Table Series.
Carrie Mae Weems, Untitled (Man Smoking/Malcolm X), from The Kitchen Table Series.
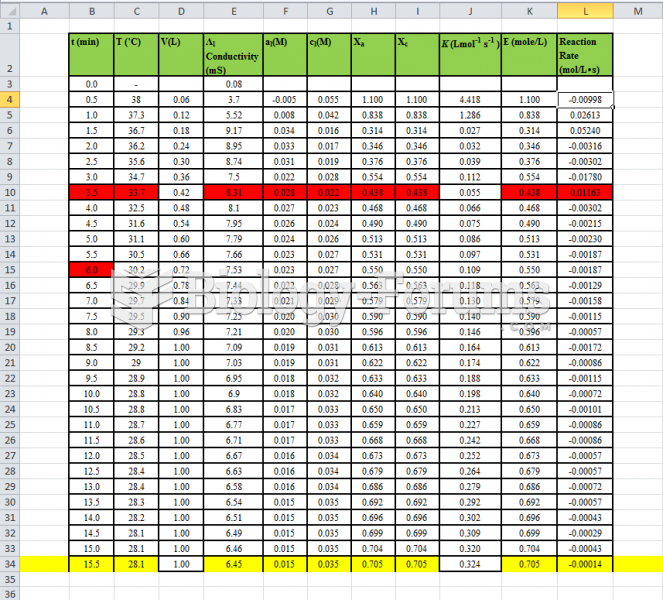 Fluidization - Data Table of experiment
Fluidization - Data Table of experiment
 How to find the first and second differences for any table of values
How to find the first and second differences for any table of values