Answer to Question 1
Most dietary strategies and drug treatments for calcium oxalate stones aim to reduce urinary calcium and oxalate levels. Dietary measures may include adjustments in calcium, oxalate, protein, and sodium intakes. Patients should consume adequate calcium from food sources (about 800 to 1200 milligrams per day) because dietary calcium combines with oxalate in the intestines, reducing oxalate absorption and helping to control hyperoxaluria. Conversely, low-calcium diets promote oxalate absorption and higher urinary oxalate levels. Some individuals with hyperoxaluria may benefit from dietary oxalate restriction. Vitamin C intakes should not exceed the RDA (90 and 75 milligrams for men and women, respectively) because vitamin C degrades to oxalate. High intakes of protein (especially from meat, fish, poultry, or eggs) and sodium increase urinary calcium excretion, so moderate protein consumption (0.8 to 1.0 gram per kilogram of body weight per day) and a controlled sodium intake (no more than about 2000 to 3000 milligrams daily) are also advised. Patients with hypocitraturia are usually advised to reduce intakes of animal proteins and increase intakes of fruits and vegetables.
Answer to Question 2
D

 Effects of Therapy for Stuttering A functional MRI scan shows regions of the superior temporal lobe
Effects of Therapy for Stuttering A functional MRI scan shows regions of the superior temporal lobe
 Educate clients about products related to massage therapy and the clients’ health goals without ...
Educate clients about products related to massage therapy and the clients’ health goals without ...
 Therapy to Prevent PTSD after Disaster
Therapy to Prevent PTSD after Disaster
 Sultan + Shepard, Le Youth - Skipping Stones
Sultan + Shepard, Le Youth - Skipping Stones
 Ex vivo and in vivo gene therapy for a patient with a liver disorder
Ex vivo and in vivo gene therapy for a patient with a liver disorder
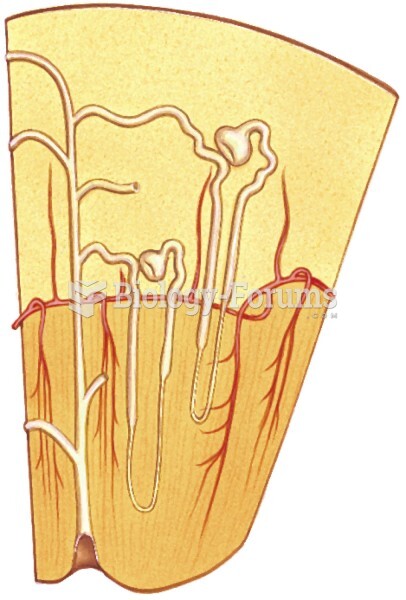 Orientation and structure of a nephron, the functional unit of the kidney.
Orientation and structure of a nephron, the functional unit of the kidney.