Answer to Question 1
(1) 48-hour pH monitoring with intraesophageal pH electrode and recorder:
This test involves placing a pH probe into the distal esophagus for a 12- to 24-hour period in order to generate a graph depicting continuous pH readings.
Information is obtained regarding quantity and pattern of gastroesophageal (GE) reflux events, the correlation with symptoms, and the efficiency of esophageal acid clearance.
(2) Barium esophagram:
A radiologist attempts to demonstrate reflux using abdominal pressure and positional changes.
In these procedures; the patient is given a contrast medium to drink. The most common medium is barium sulfate, which is a chalky, white, radiopaque substance the patient drinks like a milkshake.
The barium can be visualized by fluoroscopy or by x-ray.
This study allows the physician to monitor swallowing and the movement through the stomach into the duodenum. It also can distinguish many other abnormalities such as ulcers, tumors, or inflammation.
(3) Endoscopy with biopsy to r/o H. pylori infection:
After sedation, a fiberoptic endoscope is passed through the oral pharynx, through the esophagus, and into the stomach.
This allows the physician to visualize the anatomy of the upper gastrointestinal tract.
A needle biopsy can be passed through the endoscope, allowing for determination of the presence of microorganisms within the collected tissue.
Answer to Question 2
A systemic inflammatory response occurs after a TBI and is similar to that of burns and sepsis. The increased levels of cortisol and catecholamines (norepinephrine and epinephrine) results in a hypermetabolic response associated with increased gluconeogenesis, glycogenolysis, lipolysis, and protein wasting. Hyperglycemia and insulin resistance are also common metabolic issues associated with this inflammatory response. Due to this extreme level of catabolism, it is important to aggressively feed TBI patients to prevent excessive loss in body weight.

 The nurse needs to inform the patient with impaired vision when a touch is to occur and ask permissi
The nurse needs to inform the patient with impaired vision when a touch is to occur and ask permissi
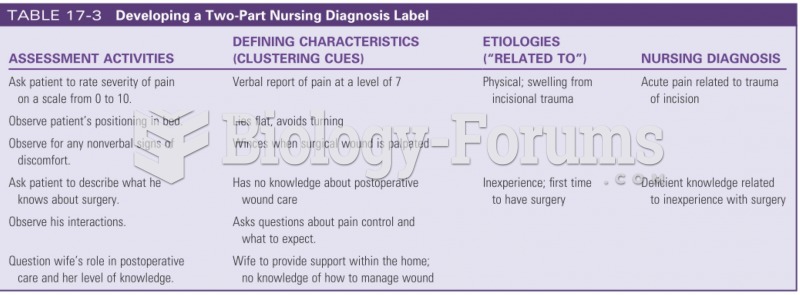 Developing a two part nursing diagnostic label
Developing a two part nursing diagnostic label
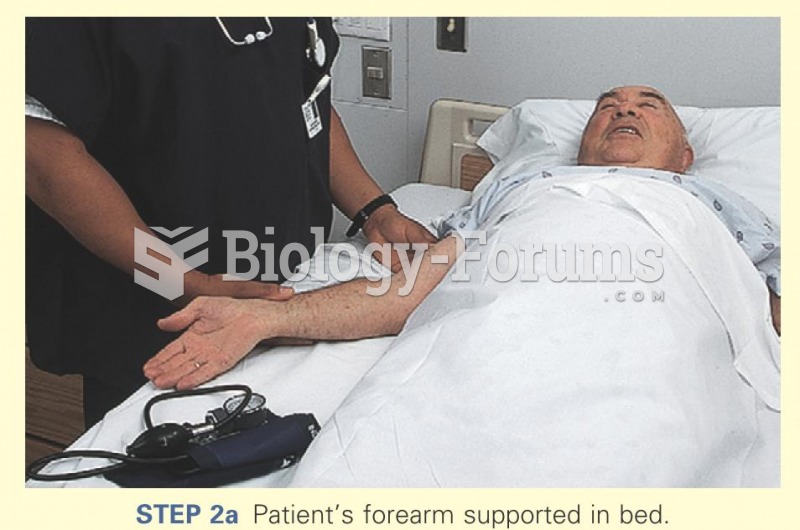 Patient's forearm supported in bed
Patient's forearm supported in bed
 The reminder card should be completed and handed to the patient after the appointment is scheduled.
The reminder card should be completed and handed to the patient after the appointment is scheduled.
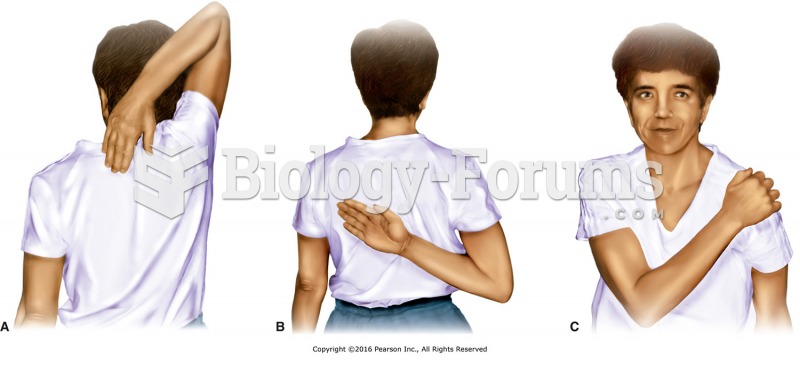 Active range of motion (AROM) tests for the shoulder. A, Apley Scratch Test. B and C, Internal ...
Active range of motion (AROM) tests for the shoulder. A, Apley Scratch Test. B and C, Internal ...
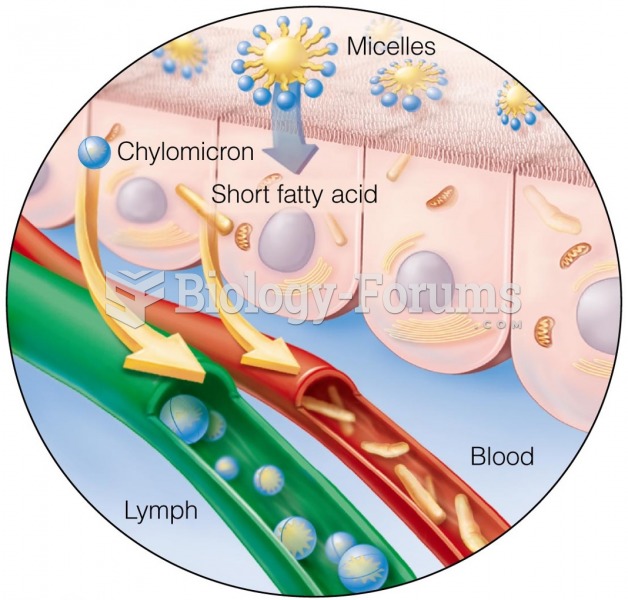 Describe how fat is digested, absorbed, and transported in the body
Describe how fat is digested, absorbed, and transported in the body