Answer to Question 1
Pre-dialysis (Stages 1-2):
0.8-1.4 g/kg
Rationale: Adequate protein to preserve muscle mass, serum proteins, and kidney function; the current evidence doesn't suggest lowering protein intake at these stages of kidney function
Pre-dialysis (Stages 3-4):
0.60-0.75 g/kg;
Rationale: Adequate protein to preserve muscle mass and serum proteins; due to a lower level of kidney function, this lower protein diet can limit the production of nitrogenous wastes and their effects on the loss of kidney function
HD:
1.2 g/kg SBW; 50 HBV
Rationale: Loss of protein during dialysis; altered albumin turnover; metabolic acidosis, which increases amino acid degradation; inflammation; and infection
PD:
1.2-1.3 g/kg SBW; 50 HBV
Rationale: Dialysate protein losses increase by 50-100 to an average of 5-15 g/day; peritonitis increases losses more to about 15-36 g/day
Note: HBV (high biological value) protein is suggested due to its similar amino acid composition to human protein and its increased utilization in the body. This should prevent the increasing nitrogenous load that protein metabolism promotes.
Answer to Question 2
Significant section of stomach bypassed, reducing gastric acid needed for promoting the ferrous state of iron (needed for absorption) and reduced intrinsic factor for B12 absorption
Additionally, gastric acid is needed to cleave many minerals and vitamins from other molecular structures and promote their absorbable forms
Duodenum and proximal jejunum bypassed, thus reducing the overall surface area and time for digestion and absorption
Lactose intolerance may transiently occur due to the production of lactase in the removed part of the small intestine; adaptation can occur
Deficiencies in fat-soluble vitamins (A, D, E, K), vitamin B12, folate, iron, and calcium are common
Other surgical procedures like the duodenal switch and biliopancreatic diversion may have similar effects due to their alterations in the GI tract pathways/release of digestive enzymes

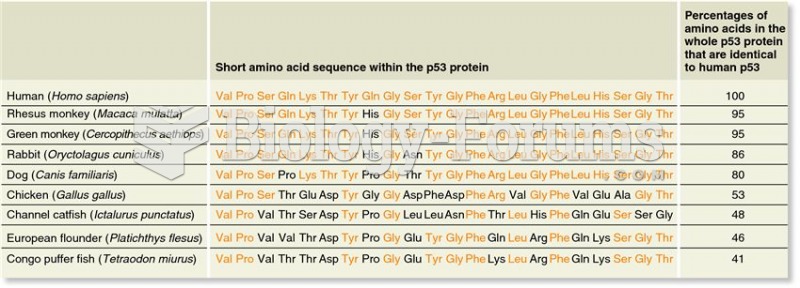 An example of genetic homology: a comparison of a short amino acid sequence within the p53 protein f
An example of genetic homology: a comparison of a short amino acid sequence within the p53 protein f
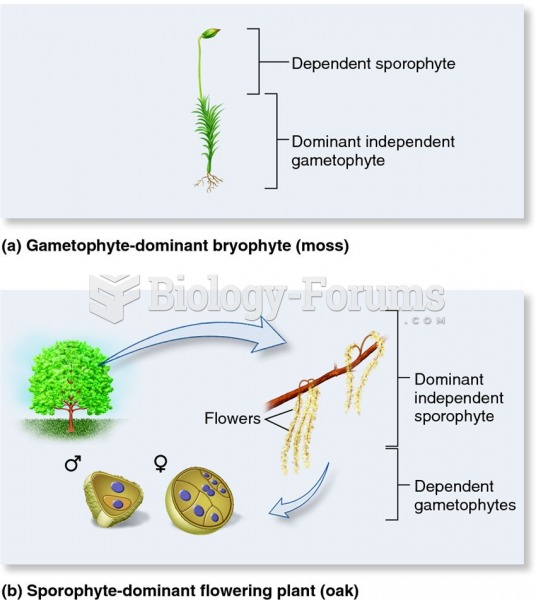 Evolutionary shift in plant life cycle stage dominance.
Evolutionary shift in plant life cycle stage dominance.
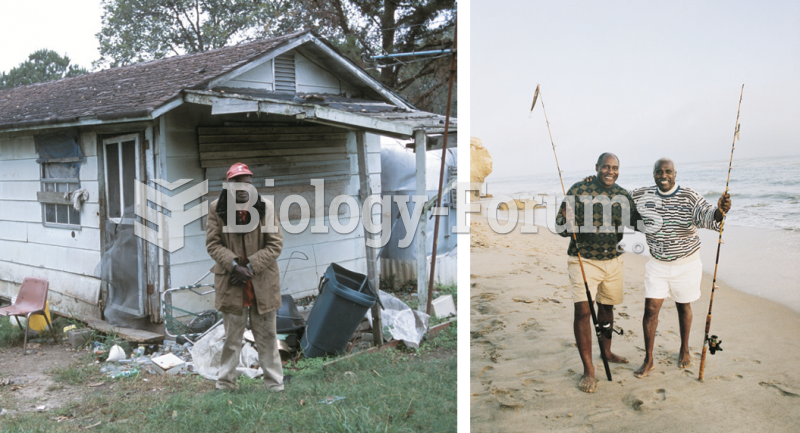 In old age, as in all other stages of the life course, people find life more pleasant if they have ...
In old age, as in all other stages of the life course, people find life more pleasant if they have ...
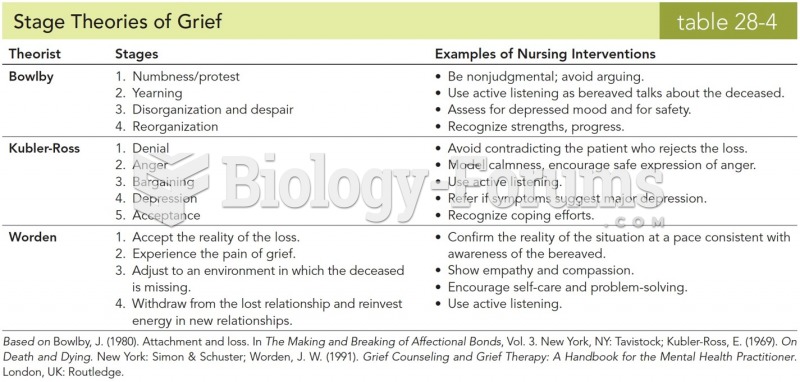 Stages Theories of Grief
Stages Theories of Grief
 Protein Synthesis
Protein Synthesis