Answer to Question 1
Normal saline delivered via an IV will restore the electrolyte imbalance that occurred due to HHS (more specifically, that occurred from osmotic diuresis). Sodium was lost during this process, which is why saline is administered. This will correct the severe state of dehydration more rapidly than drinking water.
Potassium is another electrolyte that will be out of balance with dehydration. In addition, the patient is taking Dyazide, which is not a potassium-sparing diuretic. Therefore, potassium is commonly lost when using this medication. Although patient is not taking his diabetes medications, he claims to still be taking Dyazide to help with his blood pressure. Potassium is commonly lost in the urine with osmotic diuresis. This occurred because of the serious hyperosmolar state of the blood.
The infusion of the potassium in the saline is due to the low levels of intracellular potassium. This potassium deficit is not apparent in Mitch's labs (3.9 and 4.0 mEq/L), but that is a measure of his serum levels which are typically normal or high in HHS patients. That is because the hypertonic and insulin-deficient bloodstream supports retention of potassium in the extracellular space. If potassium is not supplemented during rehydration and insulin infusion, hypokalemia will result as potassium rushes into the cells.
Insulin is used to help correct the extremely high blood glucose levels. Since the patient has low levels of circulating insulin, which is associated with HHS, insulin is needed to help insulin-dependent tissues uptake glucose.
Answer to Question 2
Since children are still growing in height, weight-loss goals should be realistic and should not necessarily attempt to fully normalize weight.
For children at risk for overweight with no identified complications, maintenance of current weight is recommended. Prolonged maintenance will allow a gradual decline in BMI units as children grow in height.
For children who are overweight and those overweight with complications, gradual weight loss is recommended.
Rate of weight loss should be based on health risks and recommended with caution. Primary goals of treatment are:
Promote healthful lifestyle behaviors to achieve and maintain a desirable body weight
Well-balanced diet that supports growth and development
Behavior modification
Increased physical activity
Family involvement
Improve/resolve complications of obesity if present
In children, generally weight loss should not exceed 2 lbs per week and this high rate of weight loss is generally reserved for the 6-11 yr olds in the 99th -tile or 12-18 yr olds with 95-tile

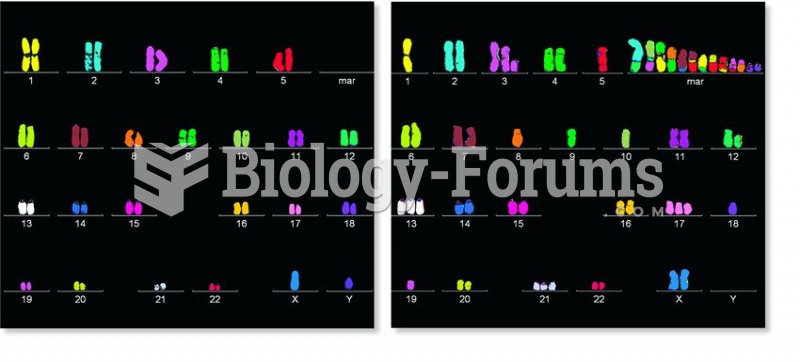 A comparison between chromosomes found in a normal human cell and a cancer cell from the same person
A comparison between chromosomes found in a normal human cell and a cancer cell from the same person
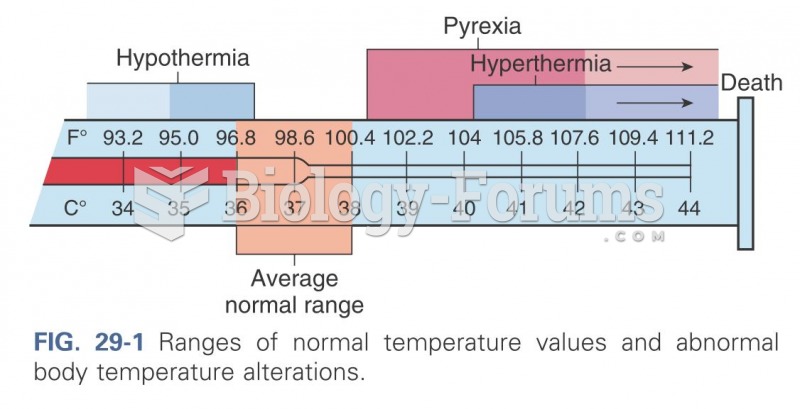 Ranges of normal temperature values
Ranges of normal temperature values
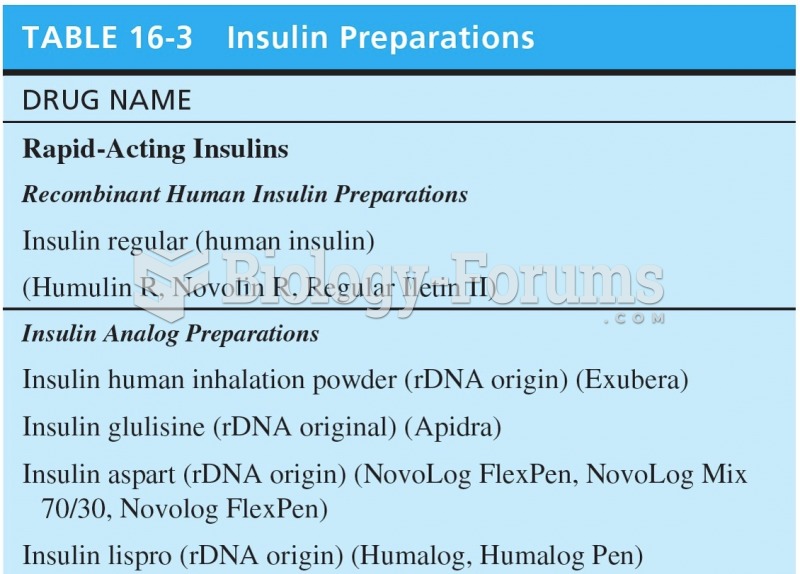 Insulin Preparations
Insulin Preparations
 Red blood cells with normal hemoglobin, like the three similar ones, are smooth and round
Red blood cells with normal hemoglobin, like the three similar ones, are smooth and round
 Normal and Impaired Vision
Normal and Impaired Vision
 In 2000, the average charge of tax preparation was 95 . Assuming a normal distribution and a ...
In 2000, the average charge of tax preparation was 95 . Assuming a normal distribution and a ...