Code the following cases for inpatient facility purposes using ICD-9-CM and ICD-10-CM and PCS codes.
Calculate the MS-DRG .
Identify the Principal vs. Secondary diagnoses and procedures.
Use external cause codes when appropriate.
Do NOT code procedures that are captured by the facility chargemaster.
Secondary diagnoses and procedures do NOT need to be sequenced in any particular order.
Enter "None" when no code is required.
If more than one occurrence of a procedure is required, report the code with "x 2""x 3" etc.
INPATIENT HOSPITAL
Health Record Face Sheet
Record Number: 76-50-77
Age: 31
Gender: Male
Length of Stay: 1 Day
Service Type: Inpatient
Discharge Status: To Home
Diagnosis/Procedure: Left Inguinal Hernia
Herniorrhaphy
DISCHARGE SUMMARY
PATIENT: WALLACE INPATIENT
Record Number: 76-50-77
ADMITTED: 06-03-XX
DISCHARGED: 06-04-XX
PHYSICIAN: DR. ALEX, M.D.DIAGNOSIS: Left inguinal hernia.
PROCEDURE: Herniorrhaphy.
HISTORY OF THE PRESENT ILLNESS: : The patient is a 31-year-old Caucasian male who was in his usual state of health until approximately 1-2 weeks prior to admission at which time he developed severe pain in his left groin following some heavy lifting. He noticed that he had swelling in his groin and presented for evaluation with a diagnosis of hernia being made.
HOSPITAL COURSE: Hospital course was uneventful with the patient returning from the recovery room in good condition. The patient was watched overnight and was afebrile on the morning of discharge. Surgical site was stable with no operative complications. Patient was in good condition on discharge to home.
DISCHARGE PLANS: Discharge to home with prescription for pain medication. Patient is to follow diet and activity instructions until follow with me in the office in three weeks.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 06-21- xx 8567
HISTORY AND PHYSICAL
PATIENT: WALLACE INPATIENT
Record Number: 76-50-77
ADMITTED: 06-03-XX
DISCHARGED: 06-04-XX
PHYSICIAN: DR. ALEX, M.D.
CHIEF COMPLAINT: Left inguinal hernia.
HISTORY OF PRESENT ILLNESS: The patient is a 31-year-old Caucasian male who was in his usual state of health until approximately 1-2 weeks prior to admission at which time he developed severe pain in his left groin following some heavy lifting. He noticed that he had swelling in his groin and presented for evaluation with a diagnosis of hernia being made.
PAST MEDICAL HISTORY: Usual childhood disease. Medical diseases: He has asthma, no other medical diseases. No previous surgery. Patient denies any injuries, allergies, medications or transfusions.
DRUG ALLERGIES: None known.
MEDICATIONS: None.
FAMILY HISTORY: Mother and father alive and well. No history of familial diseases.
SOCIAL HISTORY: He is a student. He is unmarried. Does not drink or smoke.
REVIEW OF SYSTEMS: Negative.
PHYSICAL EXAMINATION: Demonstrates a well-nourished, well-developed 31-year-old Caucasian male who appears to be approximately his stated age.
HEENT: Normal.
NECK: Supple. Trachea midline. Thyroid is normal. There are no nodes, masses or bruits in the neck. The supraclavicular and infraclavicular regions are clear.
THORAX: There is normal anterior posterior diameter to the thorax.
BREASTS: Undeveloped without masses.
LUNGS: Clear to auscultation and percussion.
CARDIOVASCULAR: Heart regular rhythm without murmur. S1, S2 are normal. No S3, S4.
ABDOMEN: Soft. Bowel sounds are normal. There is a left inguinal hernia. There are no other megaly, mass, hernias bruits.
SPINE: Straight. No CVA tenderness.
RECTAL: Not done.
EXTREMITIES, NEUROLOGICAL and VASCULAR EXAMINATIONS: Normal.
IMPRESSION: Left inguinal hernia with repair.
DR. ALEX, M.D.
Electronically signed by Dr. Alex, M.D., 06-03-xx, 124
OPERATIVE REPORT
PATIENT: WALLACE INPATIENT
RECORD NUMBER: 76-50-77
DATE OF SURGERY: 06-03-XX
SURGEON: DR. ALEX, M.D.
PREOPERATIVE DIAGNOSIS: Left inguinal hernia.
POSTOPERATIVE DIAGNOSIS: Left indirect inguinal hernia.
OPERATIVE PROCEDURE: Repair of left inguinal hernia with high ligation of the sac and Bassini reconstruction of the floor.
ANESTHESIA: General.
DESCRIPTION: After adequate sedation, the patient was brought to the operating room and placed in the supine position on the operating table. Anesthesia was induced with intravenous Pentothal, endotracheal tube was passed and the patient was maintained on endotracheal anesthesia. After obtaining proper anesthesia, the patient was prepped and draped in the usual fashion.A standard left groin incision was accomplished, carried down through subcutaneous tissue. The external oblique was divided in line with its fibers; the cord structures were carefully freed up and protected with a Penrose drain. The cremasteric muscle was incised and a large sac identified. This was very thin-walled and had the appearance of being extremely acute. The sac was carefully freed up from the surrounding tissues, twisted and high ligation accomplished with 0 silk followed by a 2-0 silk suture ligature. The sac was excised. A relaxing incision was performed in the usual fashion. Cremasteric was removed from the end of the conjoined tendon. The conjoined tendon was sutured to the shelving edge of Poupart's with interrupted 0 Marceline.The wound was irrigated with antibiotics and injected with Marcaine after which the external oblique was repaired with a continuous 3-0 Silk. The wound was then again irrigated with antibiotics after which the dermis was approximated with continuous 3-0 Vicryl and the epidermis with Steri-Strips. Sterile dressings were applied. The patient was allowed to wake up, was extubated and taken to recovery where he arrived in satisfactory condition.
DR. ALEX, M.D.
Electronically signed by Dr. Alex, M.D., 06-03-xx, 1242
PATHOLOGY REPORT
PATIENT: WALLACE INPATIENT
RECORD NUMBER: 76-50-77
DATE OF SURGERY: 06-03-XX
SURGEON: DR. ALEX, M.D.
OPERATION: Left inguinal hernia repair
GROSS DESCRIPTION: Submitted from the left inguinal region are portions of purplish-tan, membranous, fibrous connective tissue, which together measure approximately 4.5 cm. Representative portions are submitted for examination.
MICROSCOPIC DESCRIPTION: Sections reveal fibrovascular connective and adipose tissue. Portions of the tissue have a sac-like configuration with the lumen lined by mesothelium cells.
DIAGNOSIS: Hernia sac without significant features.
DR. PAT, M.D.
Electronically signed by Dr. Pat, M.D., 06-04-xx, 2245
ICD-9-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-9-CM procedure code(s): PPx_____________________
SPx_____________________
ICD-10-CM diagnosis code(s): PDx____________________
SDx _____________________
ICD-10-PCS procedure code(s): PPx_____________________
SPx_____________________
MS-DRG: _____________________

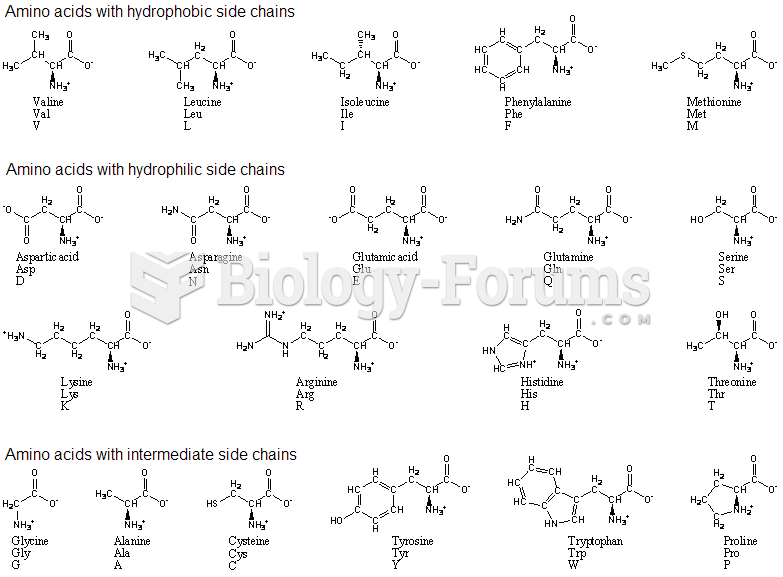 amino acids with single and three code
amino acids with single and three code
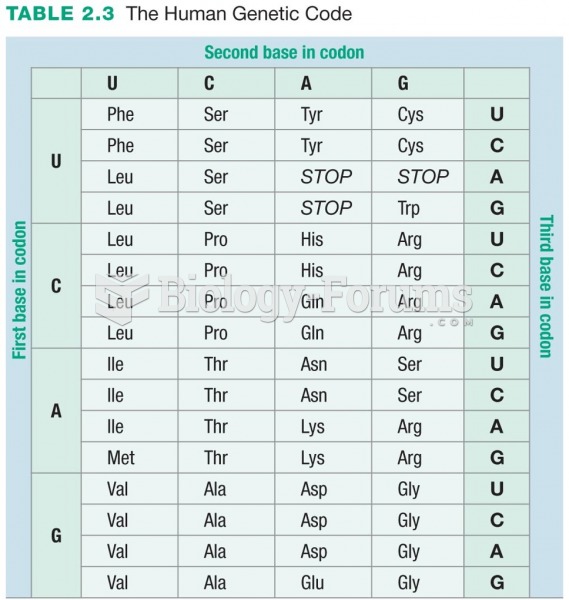 The Human Genetic Code
The Human Genetic Code
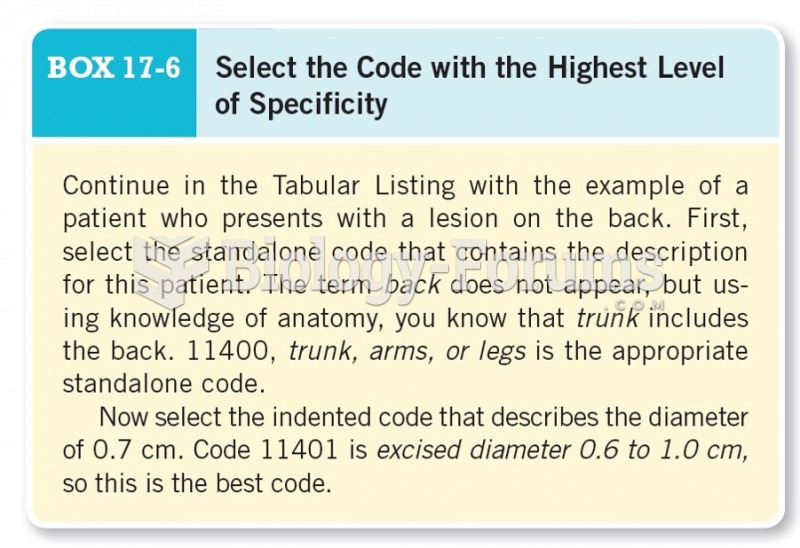 Select the Code with the Highest Level of Specificity
Select the Code with the Highest Level of Specificity
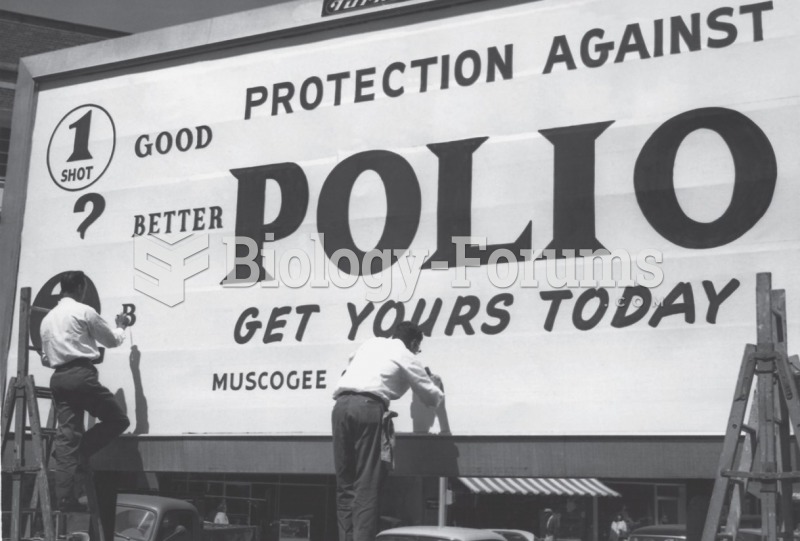 Polio eradication campaign in Georgia in the 1950s. In the 1950s, 20,000 cases of polio occurred ...
Polio eradication campaign in Georgia in the 1950s. In the 1950s, 20,000 cases of polio occurred ...
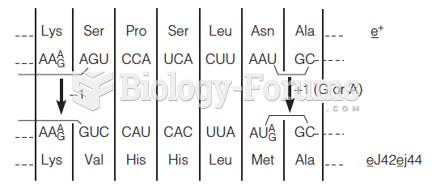 Validation of the genetic code by amino acid sequence analysis of T4 phage lysozyme mutants
Validation of the genetic code by amino acid sequence analysis of T4 phage lysozyme mutants
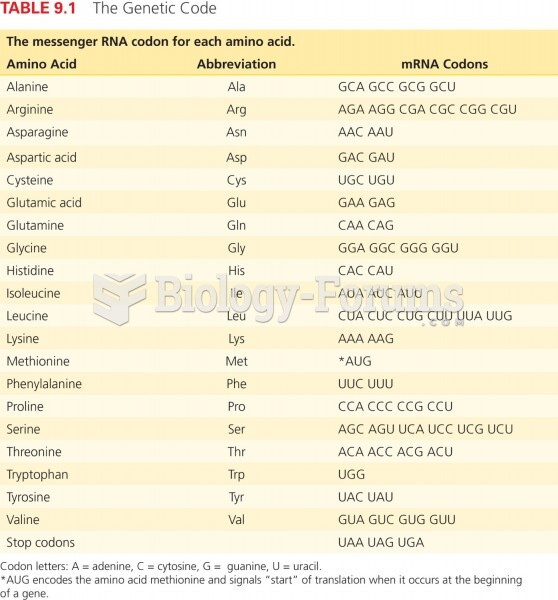 The Genetic Code
The Genetic Code