Code the following cases for inpatient facility purposes using ICD-9-CM and ICD-10-CM and PCS codes.
Calculate the MS-DRG .
Identify the Principal vs. Secondary diagnoses and procedures.
Use external cause codes when appropriate.
Do NOT code procedures that are captured by the facility chargemaster.
Secondary diagnoses and procedures do NOT need to be sequenced in any particular order.
Enter "None" when no code is required.
If more than one occurrence of a procedure is required, report the code with "x 2""x 3" etc.
INPATIENT HOSPITAL
Health Record Face Sheet
Record Number: 72-50-77
Age: 79
Gender: Female
Length of Stay: 5 Days
Service Type: INPATIENT
Discharge Status: To Home
Diagnosis/Procedure: Colon Cancer.
Partial Colectomy.
DISCHARGE SUMMARY
PATIENT NAME: Cassandra Inpatient
RECORD NUMBER: 72-50-77
ADMISSION DATE: 05-02-xx
DISCHARGE DATE: 05-7-xx
PHYSICIAN: DR. TONY, M.D.
DISCHARGE DIANOSIS:
1. Colon cancer, specifically adenocarcinoma.
PROCEDURES:
1. Partial colectomy.
HOSPITAL SUMMARY: The patient is a 79-year-old white widow who was admitted to the hospital for workup of some abdominal pain. She had been having trouble for several weeks and been going downhill. Her appetite had been bad. She was brought into the hospital initially for workup and part of that workup included a barium enema, which showed a constricting annular lesion of the colon. At that point, the patient was seen by an internist, who evaluated the patient. After transfusing some blood to build up her hematocrit, she was taken to surgery electively and underwent a partial colectomy for treatment of this condition.
Her postoperative course was excellent and she was able to be discharged temporarily to a nursing home to continue her recovery. Please see full operative dictation for complete details of the surgical procedure.
_____________________________
Tony Surgeon, M.D.
HISTORY AND PHYSICAL
PATIENT NAME: Cassandra Inpatient
RECORD NUMBER: 72-50-77
ADMISSION DATE: 05-02-xx
DISCHARGE DATE: xx-xx-xx
PHYSICIAN: DR. TONY, M.D.
CHIEF COMPLAINT: Abdominal pain and fullness.
HISTORY OF PRESENT ILLNESS: This is a 79-year-old white female who has been ill for the past several days with abdominal pain and bloating, even some diarrhea on the day prior to admission. She thought that maybe she had just had the stomach flu, but when she did not get better, she was brought to the office for an examination. At that time, the patient looked pale and she was admitted to short stay initially for work up. The patient had been known to be anemic recently and been taking some iron pills for that. She denied any blood in the stool or any blood in the urine or any place else.
PAST MEDICAL HISTORY:
1. History of anemia.
2. She has a history of obstructive hydrocephalus that was due to an arachnoid cyst and she did undergo ventriculo-peritoneal shunt placement for that.
3. She also has a history of psoriasis.
PAST SURGICAL HISTORY: She has had a hysterectomy, appendectomy and the shunt placement as mentioned above for the hydrocephalus. She also had a laminectomy for spinal stenosis. I believe the shunt placement in her head was in inserted earlier in the year.
MEDICATIONS: Besides some topical ointment for psoriasis and iron for the anemia, she is not on any medications.
ALLERGIES: No known drug allergies.
SOCIAL HISTORY: She does not smoke or drink. She used to smoke, but quit about 30 years ago. The patient is a widow. She lost her husband to heart problems.
REVIEW OF SYSTEMS: She has lost some weight over the past several months. She is not sure exactly how many pounds. She has been progressively getting weaker in the past several months as well.
PHYSICAL EXAMINATIONGENERAL: She presents as a pale appearing white elderly female. She is in no acute distress.VITAL SIGNS: Normal with a temperature of 98.6°F.
HEENT: Negative, excepting pale mucous membranes of the eyes and oral mucoua.
NECK: Supple with no masses.
CHEST: Lungs are clear.
CARDIOVASCULAR: Heart is regular. No murmurs or gallops.BREASTS: Not examined at this time.
ABDOMEN: Soft. It is tender to palpation in all quadrants. Definite mass is felt to palpation.
EXTREMITIES: Extremities show no cyanosis, clubbing or edema.
INITIAL IMPRESSION:
1. Abdominal pain of unknown cause. I have a suspicion that this patient may have some sort of occult malignancy with the weight loss and anemia, specifically colon cancer.
PLAN: Admission and workup of these problems.
DR. TONY, M.D.
Electronically authenicated by Dr. Tony, 05-07-xx 6789
OPERATIVE REPORT
PATIENT NAME: Cassandra Inpatient
RECORD NUMBER: 72-50-77
OPERATION DATE: 05-02-xx
SURGEON: Dr. Tony, M.D.
PREOPERATIVE DIAGNOSIS: 1. Adenocarcinoma of the hepatic flexure of the colon.
2. Cholecystitis and cholelithiasis.
POSTOPERATIVE DIAGNOSIS: 1. Adenocarcinoma of the hepatic flexure of the colon.
2. Cholecystitis and cholelithiasis.
PROCEDURE PERFORMED: Right hemi colectomy, cholecystectomy.ANESTHESIA: General.
DESCRIPTION OF PROCEDURE: The patient was brought to the operating room with IV infusing. Preoperative antibiotics administered. General anesthesia was induced. Nasogastric tube and Foley catheter were inserted. The abdomen was prepped with Betadine sterilely.
Skin marker was used to outline a transverse upper abdominal incision beginning in the right mid abdomen laterally and extending toward the epigastrium. Skin incision was made with a #10 blade and carried through subcutaneous tissue to expose fascia. Bleeding was controlled with electrocautery. Oblique muscles were divided with electrocautery as is the rectus muscle exposing the peritoneum. The peritoneum was identified and entered. Manual and visual exploration of the abdominal cavity reveals tumor in the hepatic flexure of the colon without obvious extension into pericolonic tissues.
The gallbladder is chronically inflamed and contains stones. Retractor was positioned. With traction on the fundus of the gallbladder, the peritoneum overlying the hepato-duodenal ligament is incised. By blunt dissection, the cystic duct is skeletonized, doubly clipped and divided. Similarly, the cystic artery is bluntly dissected, doubly clipped and divided. With traction on the divided duct, the gallbladder is dissected from the liver bed with the use of the electrocautery. Specimen is submitted for pathologic evaluation. Pack was placed into the liver bed and removed after approximately 10 minutes and there is no evidence of bleeding from this surface.
Attention is then turned to the colon section. The lateral peritoneal reflection is incised with Metzenbaum scissor and the colon is reflected medially. By blunt dissection, the mesentery is elevated from the retroperitoneum.
The right ureter is identified and preserved. Point of division is chosen in the distal ileum and a GIA stapler is passed and fired. Similarly, a point in the mid transverse colon is chosen for division and a GIA stapler passed and fired. Peritoneum overlying the mesentery is incised with the Metzenbaum scissor. Mesentery is then divided between clamps and 20 silk ties and the right colon is submitted for pathologic evaluation. Area of dissection is irrigated and examined carefully for hemostasis prior to anastomosis. The small bowel was juxta opposed against the transverse colon and secured in place with 0 muscular 2-0 silk-interrupted suture. An enterotomy is made in the small bowel and colon and the GIA stapler is passed and fired forming the anastomosis. Enterotomy is then closed in two layers. The first layer is a running 3-0 chromic full thickness suture and the second is an interrupted 0 muscular 3-0 silk suture. Mesentery is then closed using a running 2-0 Vicryl suture. The area of dissection is examined carefully for hemostasis prior to closure following correct sponge, needle and instrument counts the abdomen is closed. Posterior fascia is approximated using a running suture of #1 Vicryl. The anterior rectus sheath and external oblique muscles are approximated using a running #1 Vicryl suture reinforced at intervals with #1 Prolene. Subcutaneous layer was irrigated and examined for hemostasis. Scarpa's fascia was then approximated using interrupted 2-0 Vicryl suture. Skin is approximated with skin stapler. Dry sterile dressings were applied.
The patient tolerated the procedure well and was transferred to the recovery room in stable condition.
DR. TONY, M.D.
Electronically authenicated by Dr. Tony, 05-07-xx 6789
PATHOLOGY REPORT
PATIENT NAME: Cassandra Inpatient
RECORD NUMBER: 72-50-77
OPERATION DATE: 05-02-xx
SURGEON: Dr. Tony, M.D.
SPECIMEN SUBMITTED 1. Gallbladder. 2. Right side of colon and terminal ileum.
TISSUE REPORT
HISTORY: CA of colon.
Gross 2:
Right side of the colon including attached terminal ileum and right side of colon without the appendix. The terminal ileum is 10 cm in length. It has a fairly smooth but granular serosal surface, a firm wall, a mucosa that is folded and light green. The segment of colon is 35 cm in length, includes cecum, ascending and transverse segments of the colon. In the ascending portion of the colon there is a somewhat pedunculated irregular polyp 55 x 40 x 30 mm; the surface is folded and light grey but the center is superficially ulcerated, granular and light grey. The cut section of this lesion reveals it appears to be confined to the mucosa although in the center there is a suggestion that the lesion infiltrates into the muscle coat. 5 cm distal to this polypoid lesion in the region of the transverse segment of the colon there is a 7 cm in length 4 cm in width circumferential penetrating and perforating polypoid tumor that extends to the muscle coat and into the serosal adipose tissue. The margins around the area of penetration are thickened, granular, polypoid, grey to red infected. On cut section of the mesentery in this region, it also infiltrates into the attached mesenteric adipose tissue. 6 cm distal to this lesion and approximately 3 cm from the distal resection margin there is an additional pedunculated polyp 15 x 5 x 3 mm. The cut section of the mesentery reveals eleven firm light gray lymph nodes several of which appear to be obviously replaced by firm light gray tumor. The lymph nodes are more or less discrete, the largest 15 mm in diameter.
Sections of terminal ileum one block.
Sections of the most proximal polypoid lesions.
Sections of large penetrating lesion.
Sections of most distal polypoid lesion.
Sections of mesenteric lymph nodes.
Gross 1. Gallbladder 7 x 4 x 2 cm. The surface of the gallbladder is smooth appears to be slightly thickened. The mucosa is green; the lumen contains about 10 and numerous mulberry green gallstones, the largest 5 mm in diameter.
MICROSCOPIC:
1. Gallbladder reveals changes of chronic cholecystitis.
2. Normal terminal ileum tubulovillous adenoma the center of which has infiltrated into the muscle coat.
3. The most proximal polypoid lesion reveals a well-differentiated adenocarcinoma. Lesion 5 cm distal to the polypoid area reveals a poorly differentiated adenocarcinoma composed of malignant epithelial cells having vacuola and cytoplasm arranged in cords and nests or solid sheets. This shows evidence of having provoked a rather prominent desmoplastic response extensively infiltrating the muscle coat into the serosal surface and the attached mesenteric adipose tissue. The mesenteric adipose tissue immediately adjacent to the area where the lesion has infiltrated into the mesenteric adipose tissue reveals areas thickened by proliferated fibrous connective tissue containing lymphocytes. No definite involvement in these areas can be identified.
4. The most distal polyp reveals a benign tubulovillous adenoma.
5. The sections of the 11 mesenteric lymph nodes 2E reveal, basically hyperplastic lymph nodes without any evidence of metastases. Sinusoids contain plasma cells or a few giant cells.
DIAGNOSIS: Cholecystitis, chronic.
1. Calculus, multiple right side of colon and terminal ileum.
2. Adenocarcinoma, poorly differentiated, proximal portion, transverse segment of colon.
3. Lesion infiltrates into the serosal surface and the mesenteric adipose tissue.
4. Adenocarcinoma, well-differentiated, mucosa, ascending portion of the colon.
5. Adenocarcinoma infiltrates into the superficial muscle coat.
6. Polyp, adenomatous or tubular type, distal portion, transverse segment of the colon.
7. Lymph nodes, hyperplastic, multiple (11), mesentery, right side of the colon.
8. Segment, terminal ileum, normal.
COMMENT: This 79- year-old female in the proximal transverse segment of the colon has a 7 cm in length 4 cm in width circumferential penetrating and perforating polypoid lesion that extended right to the serosal surface and the adipose tissue. On microscopic examination, this is a poorly differentiated adenocarcinoma of colonic mucosa. 11 adjacent lymph nodes were isolated and are free of metastases. In addition proximal to this adenocarcinoma there was a 55 mm polyp in the ascending portion of the colon the center of which reveals development of an early well-differentiated adenocarcinoma of colonic origin infiltrating into superficial muscle coat.
Pathological stage: T3 No MO, modified Duke's 82.DR. PAT, M.D.
Electronically authenticated by Dr. Pat, M.D. 05-03-xxx 4322
ICD-9-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-9-CM procedure code(s): PPx_____________________
SPx_____________________
ICD-10-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-10-PCS procedure code(s): PPx_____________________
SPx_____________________
MS-DRG: _____________________

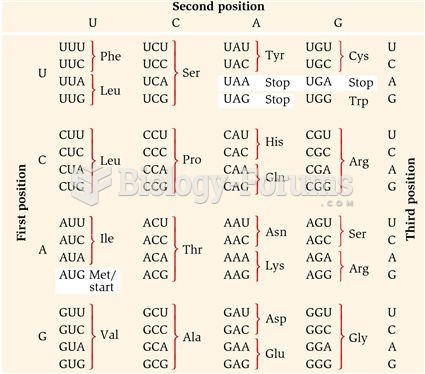 The Genetic Code
The Genetic Code
 An elephant can use its trunk for a variety of purposes. This one is wiping its eye.
An elephant can use its trunk for a variety of purposes. This one is wiping its eye.
 The vehicle’s fuel pump is disabled by removing its relay or fuse. In some cases, it may be ...
The vehicle’s fuel pump is disabled by removing its relay or fuse. In some cases, it may be ...
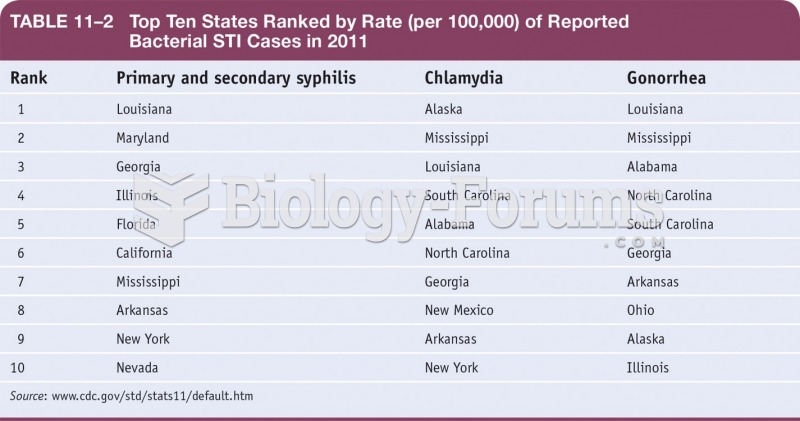 Top Ten States Ranked by Rate or Reported Bacterial STI Cases in 2011
Top Ten States Ranked by Rate or Reported Bacterial STI Cases in 2011
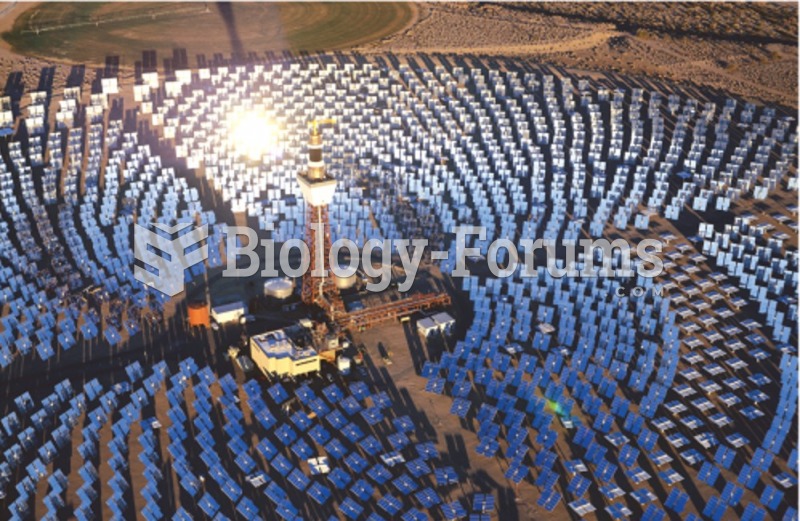 Power-tower in Southern California, largest such facility in the world
Power-tower in Southern California, largest such facility in the world
 Genomes Using Modifications of the Universal Genetic Code
Genomes Using Modifications of the Universal Genetic Code