Question 1
Which setting uses APCs for Medicare reimbursement?
◦ Physician offices
◦ Inpatient hospitals
◦ Same-day surgery
◦ Critical access hospitals
Question 2
Code the following cases for inpatient facility purposes using ICD-9-CM and ICD-10-CM and PCS codes.
Calculate the MS-DRG.
Identify the principal vs. secondary diagnoses and procedures.
Use external cause codes when appropriate.
Do NOT code procedures that are captured by the facility chargemaster.
Secondary diagnoses and procedures do not need to be sequenced in any particular order.
Enter "None" when no code is required.
INPATIENT HOSPITAL
Health Record Face SheetRecord Number: 75-50-77Age: 25Gender: Female Length of Stay: 3 Days Service Type: Inpatient Discharge Status:
To HomeDiagnosis/Procedure: Abdominal Adhesive DiseaseLaparoscopic Lysis of Adhesion with BiopsyDISCHARGE SUMMARYPATIENT: MARY INPATIENT RECORD NUMBER: 75-50-77ADMITTED: 11-04-XXDISCHARGED: 11-06-XXPHYSICIAN: DR. ALEX, M.D.ADMITTING DIAGNOSIS
: Persistent pelvic pain.
DISCHARGE DIAGNOSIS
: Abdominal adhesive disease, probable right salpingitis versus chronic interval appendicitis.
HOSPITAL COURSE: The patient is a 25-year-old white female with persistent right lower quadrant pain. She underwent IV antibiotic therapy approximately 2½ weeks ago with incomplete resolution and subsequent return of her pain. She underwent laparoscopy, at which time adhesions of the right lower quadrant involving the cecum, appendix, small bowel, right ovary, fallopian tube, and omentum were encountered. Adhesiolysis was performed, appendectomy performed, right ovarian biopsy. She was maintained on IV antibiotics for 24 hours and subsequently discharged to home.
The patient was discharged to home with instructions to follow up. She will be discharged with saline lock and maintenance to follow up in the emergency room tomorrow for an additional dose of Rocephin and have the saline lock discontinued at that time. She will continue of Vibramycin, 100 mg b.i.d., and follow up with me in the clinic in 1 week. Instructions were given on activities, bowel care and precautions.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 11-07-xx , 3343
HISTORY AND PHYSICALPATIENT: MARY INPATIENT RECORD NUMBER: 75-50-77ADMITTED: 11-04-XXDISCHARGED: 11-06-XXPHYSICIAN: DR. ALEX, M.D.CHIEF COMPLAINT: Abdominal adhesive disease, probable right salpingitis versus chronic interval appendicitis.
HISTORY OF PRESENT ILLNESS:
This is a 25-year-old white female with a history of right pelvic pain. She had initial flare approximately three weeks ago and was given 5 days of IV antibiotic followed by a week of po antibiotic and had near but not complete resolution of her pain. It was associated with some GI complaints, though not notable. Ultrasound was performed which showed a generous sized right ovary consistent with oophoritis or normal variant. The patient is quite large. Appendix was not visualized. She is not status post-operative laparoscopy with lysis of adhesions, appendectomy, ovarian biopsy, and tubal dye perfusion. She tolerated it well but because of previous infection and likelihood of involved infection, she is kept for further antibiotic therapy.
ALLERGIES: No Known Allergies
MEDICATIONS
: Proventil inhaler prn, Voltaren, 50 mg, one to two q. 6 hours, Lortab and Vibramycin.
PAST HISTORY
: She has chronic hypertension and obesity. She had a cesarean section in January of 1995.
FAMILY HISTORY:
Significant for malignancy of her father, specifics unknown, as well as some hypertension.
SOCIAL HISTORY:
She smokes greater than one pack per day, denies significant use of alcohol or recreational drugs.
REVIEW OF SYSTEMS: Negative.
PHYSICAL EXAMINATION:
VITAL SIGNS: Blood pressure 140/90. She is afebrile.
GENERAL: Alert and appropriate. Skin is clear.
HEENT/NECK: Unremarkable.
LUNGS: Clear to auscultation with decreased pulmonary excursion secondary to habitus.
CARDIOVASCULAR: Regular rate and rhythm.
ABDOMEN: Soft. Bowel sounds are normal. Incisions are dry.
EXTREMITIES: Unremarkable.
GENITORECTAL: Unremarkable.
IMPRESSION: Persistent right pelvic pain.
RECOMMENDATIONS: Proceed with a laparoscopic evaluation.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 11-04-xx , 3343
OPERATIVE REPORT PATIENT: MARY INPATIENT RECORD NUMBER: 75-50-77DATE OF SURGERY: 11-04-XXSURGEON: DR. ALEX, M.DPREOPERATIVE DIAGNOSIS: Persistent right pelvic pain.
POSTOPERATIVE DIAGNOSIS: Abdominal pelvic adhesive disease.
Chronic interval appendicitis versus chronic P.I.D. versus endometriosis.
OPERATIVE PROCEDURE: Laparoscopy with lysis of adhesions.
Right ovarian biopsy.
Tubal dye perfusion.
Appendectomy.
INTRAOPERATIVE FINDINGS: The right ovary was large and boggy, approximately 6 cm. in greatest dimension. It was swollen, lacking superficial convolutions. The appendix was involved with fat wrapping and adhesions to the pelvic brim, which also included distal right fimbria, large and small bowel, as well as omentum. The left ovary was normal size, consistency, normal convolutions, stigma of ovulation. Left fallopian tube was normal as was the uterus, vesicouterine plicae, and peritoneum of the pelvis including the ovarian fossa bilaterally. Upper abdominal sweep was unremarkable.
DESCRIPTION: With patient under general anesthetic and in dorsal lithotomy position, suitably prepped and draped with bladder drained with straight catheter, a Kroner uterine manipulator was placed. A pneumoperitoneum was created and trocar placed. Additional trocars in the suprapubic bilateral space were placed under direct visualization. The upper abdominal sweep showed findings as listed at the right pelvic brim. The patient was placed in gentle Trendelenburg and left tilt. Adhesiolysis was carried out until the base of the appendix was freed. The right fallopian tube was also freed, as was the right ovary. A right ovarian wedge biopsy was carried out and specimen submitted. An Endo-GIA was used to perform an appendectomy with sharp and blunted adhesiolysis to the appendiceal stump and a single white endostaple placed across the appendiceal stump. Hemostasis was immediate. Copious irrigation was undertaken. Additional adhesiolysis was performed involving the large and small bowel.
The left ovary and remainder of pelvis was visualized and peritoneum again was noted to be normal. No alterations or distortions of the superficial vasculature. No scarring throughout the cul-de-sac, anterior vesicouterine plicae. Tubal dye perfusion was then performed and easy spill noted bilaterally. Irrigation was again carried out. Inferior trocars were removed and remained hemostatic. Abdominal trocar was removed. Pneumoperitoneum was allowed to escape. Sutures were placed in the fascia on the 10 or greater trocar sites and subcuticular stitches of 4-0 un-dyed Vicryl used to approximate the skin. Instrumentation was removed from the vagina. Dressings were applied. Patient was taken to the recovery room in stable condition.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 11-04-xx, 3343
PATHOLOGY REPORT PATIENT: MARY INPATIENT
RECORD NUMBER: 75-50-77
ADMITTED: 11-04-XX
PHYSICIAN: DR. ALEX, M.D
OPERATION: Laparoscopy with lysis of adhesions, right ovarian biopsy, tubal dye perfusion, and appendectomy.
GROSS DESCRIPTION: The tortuous appendix is 11 cm in length, 5 mm in width and blends with abundant mesoappendix. The serosal surface of the appendix is smooth; the wall is firm; the lumen contains firm brown fecal material.
The specimen labeled ovarian biopsy consists of two irregular portions of light grey or dark red hemorrhagic tissue, the larger 25 x 10 x 5 mm.
MICROSCOPIC DESCRIPTION: The entire appendix was examined microscopically and there is no evidence of an acute, sub-acute appendicitis. There is also no evidence of a periappendicitis such as one might expect to find in pelvic inflammatory disease. The ovarian biopsy simply reveals normal ovarian stroma containing a few primordial follicles.
DIAGNOSIS: 1.
Appendix normal.
2. Segment, ovary, normal, right side.DR. PAT, M.D.
Electronically authenticated by Dr. Pat, 11-05-xx, 4432ICD-9-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-9-CM procedure code(s): PPx_____________________
SPx_____________________
ICD-10-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-10-PCS procedure code(s): PPx_____________________
SPx_____________________
MS-DRG: _____________________

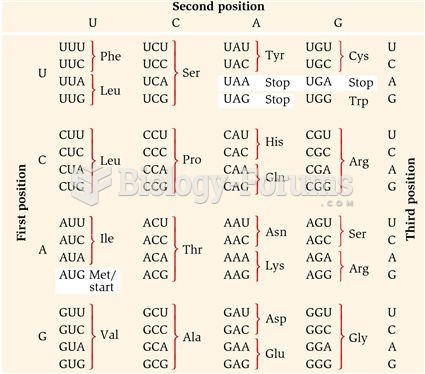 The Genetic Code
The Genetic Code
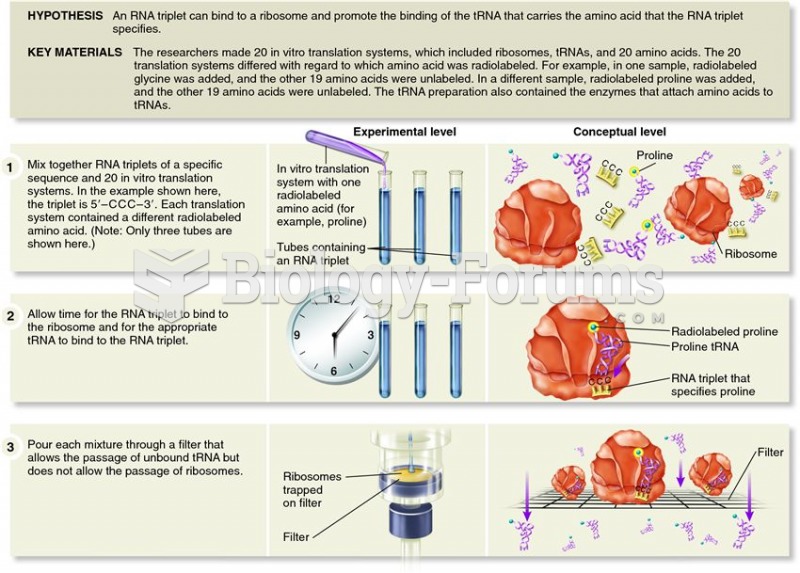 Nirenberg and Leder's use of triplet binding assays to decipher the genetic code
Nirenberg and Leder's use of triplet binding assays to decipher the genetic code
 USF Biologist Taegan McMahon conducts experiments on chlorothalonil at a research facility in East H
USF Biologist Taegan McMahon conducts experiments on chlorothalonil at a research facility in East H
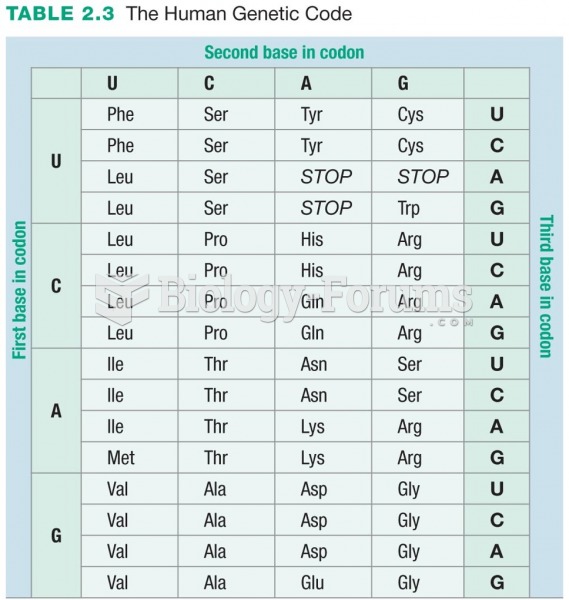 The Human Genetic Code
The Human Genetic Code
 Review Bundling, Add-on Codes, and Quantity Edits
Review Bundling, Add-on Codes, and Quantity Edits
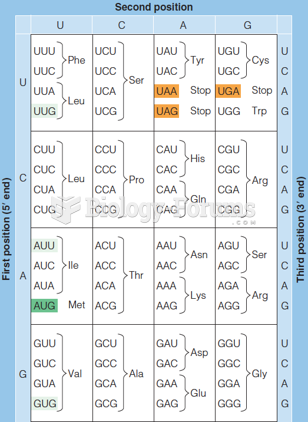 The genetic code (as written in RNA)
The genetic code (as written in RNA)