This topic contains a solution. Click here to go to the answer
|
|
|

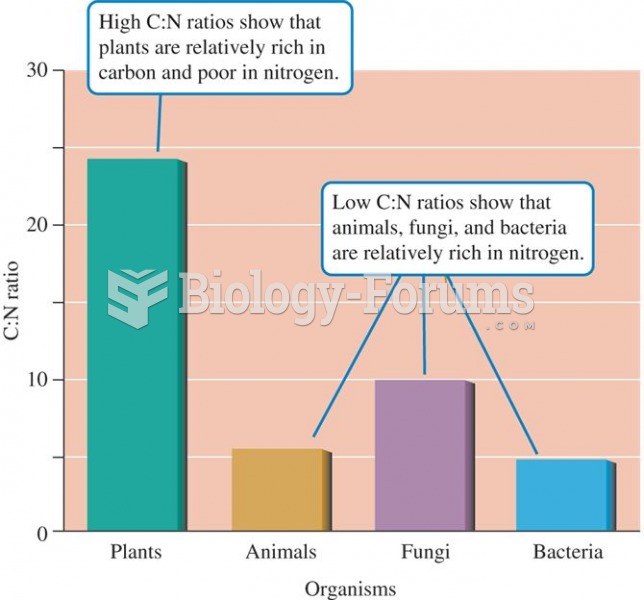 On average, the ratio of carbon to nitrogen is much higher in terrestrial plants than in other major
On average, the ratio of carbon to nitrogen is much higher in terrestrial plants than in other major
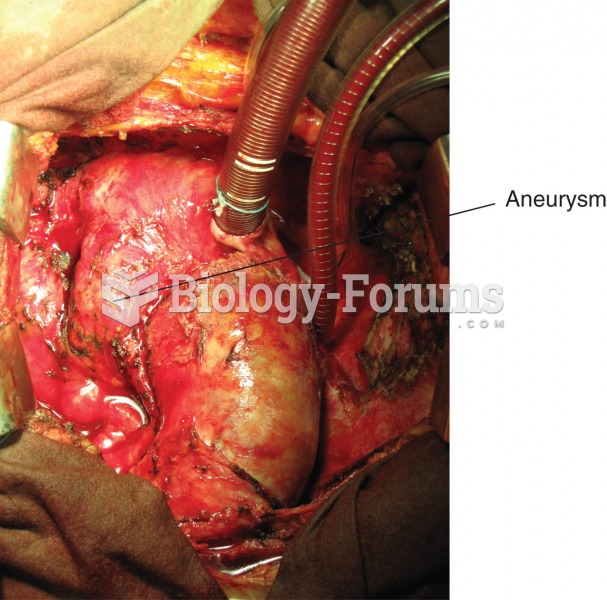 Aneurysm. Photograph of the aorta, the large blood vessel arising from the heart, with a large bulge
Aneurysm. Photograph of the aorta, the large blood vessel arising from the heart, with a large bulge
 Social Problems: A Critical Power-Conflict Perspective
Social Problems: A Critical Power-Conflict Perspective
 International space station
International space station
 International space station
International space station
 Test-Cross Results from Mendel’s Experiments
Test-Cross Results from Mendel’s Experiments