Answer to Question 1
ANS: D
Monitoring FHR is a vital component of fetal surveillance, as it provides important information on placental function, fetal hypoxia, and whether the intrauterine environment can support and sustain the fetus. The FHR can usually be auscultated as early as 10 weeks with an electronic Doppler and by 16 to 19 weeks with careful assessment and fetoscope (Cunningham et al., 2010). A normal FHR is 120 to 160 beats per minute. A sustained FHR of below 100 beats per minute is indicative of fetal jeopardy. If there is a question of whether the FHR is being adequately evaluated, the maternal pulse should simultaneously be assessed to ensure that the FHR, not the maternal heart rate, is actually being auscultated.
Answer to Question 2
ANS: A
The reproductive history includes the contraceptive, sexual, and obstetric history. The contraceptive history elicits the last time contraceptives have been used, what types of contraceptives were used, and the dates of any unprotected intercourse. The sexual history helps identify risks for sexually transmitted diseases (STDs) or ectopic pregnancies. The obstetric history consists of the number of pregnancies and their outcomes using the gravidaparaTPAL nomenclature (Table 19.1). This portion of the history also includes the year of each pregnancy, infant birth weight, gestational age at birth, type of delivery (vaginal or caesarean), length of labor, anesthesia received, and any maternal or fetal complications during the pregnancy. Gravida indicates the number of pregnancies. Para indicates the number of pregnancies that surpassed 20 weeks. In TPAL, T indicates term pregnancies, P indicates premature births, A indicates abortions (spontaneous or induced), and L indicates live births.

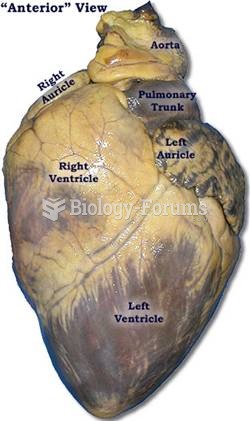 SHEEP HEART
SHEEP HEART
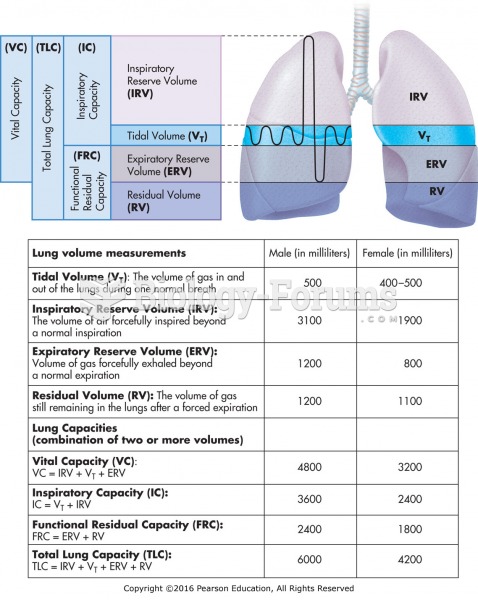 Normal lung volumes and capacities.
Normal lung volumes and capacities.
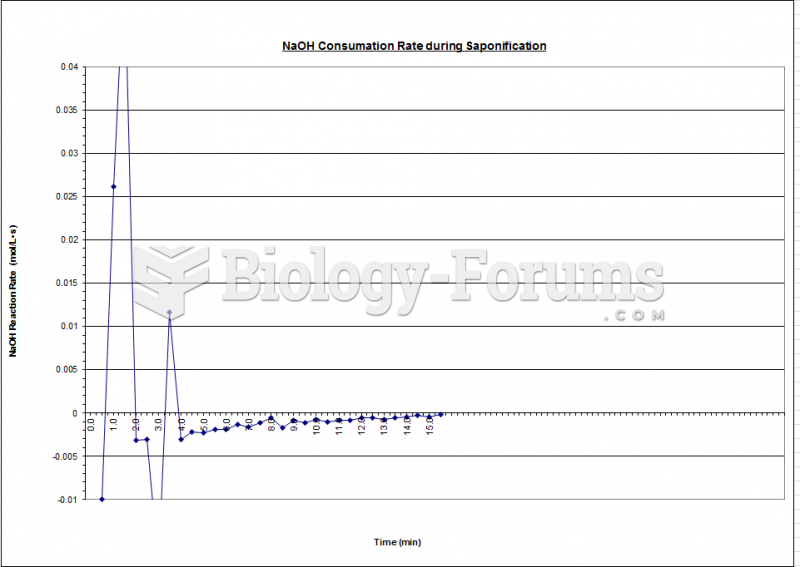 Fluidization - Reaction Rate Chart
Fluidization - Reaction Rate Chart
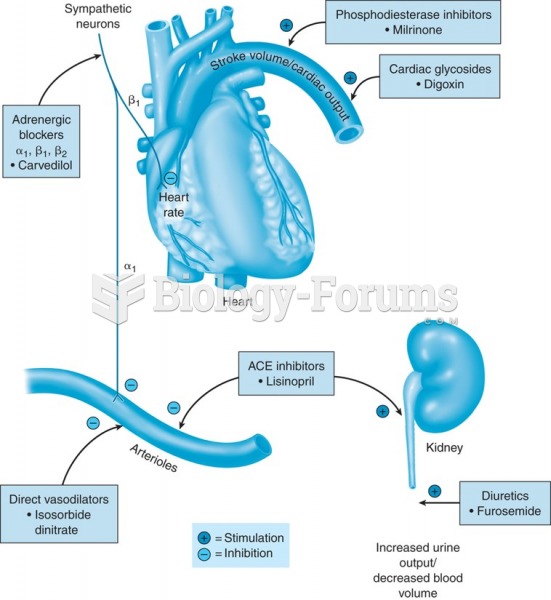 Mechanisms of action of drugs used for heart failure.
Mechanisms of action of drugs used for heart failure.
 Positions for auscultation of the heart: Lateral
Positions for auscultation of the heart: Lateral
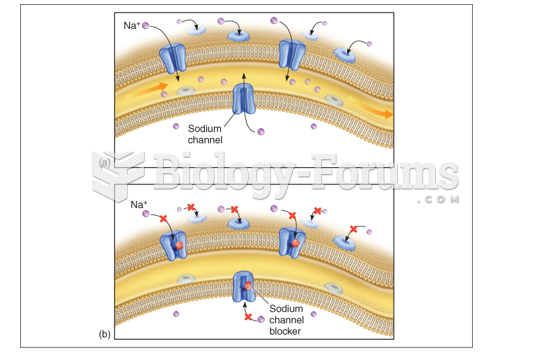 Normal nerve conduction of Sodium ion
Normal nerve conduction of Sodium ion