Answer to Question 1
B
The electrocardiographi c tracing in atrial fibrillation is notable for an uneven atrial baseline that lacks clearly defined P waves and instead shows rapid oscillations or fibrillatory wavelets that vary in size, shape, and frequency. Junctional escape rhythm has a rate of 40 to 60 beats/min and regular rhythm but P waves maybe present or absent, inverted in lead II, PR interval less than 0.12 sec, and QRS complex is 0.06 to 0.10 seconds. With premature ventricular contractions, the QRS can manifest in an unlimited number of shapes or patterns. If all of the ventricular ectopic beats look the same in a particular lead, they are called unifocal, which means that they probably all result from the same irritable focus. Ventricular tachycardia is caused by a ventricular pacing site firing at a rate of 100 times or more per minute, usually maintained by a re-entry mechanism within the ventricular tissue. The complexes are wide, and the rhythm may be slightly irregular, often accelerating as the tachycardia continues.
Answer to Question 2
C
Tracheal deviation and jugular venous distention are findings associated with tension pneumothorax. Respiratory acidosis is usually present because of the ineffective breathing pattern. In a flail chest, a free-floating segment of the chest wall moves independently from the rest of the thorax and results in paradoxical chest wall movement during the respiratory cycle. During inspiration, the intact portion of the chest wall expands while the injured part is sucked in. During expiration, the chest wall moves in, and the flail segment moves out.

 Unique markings identify individual humpback whales.
Unique markings identify individual humpback whales.
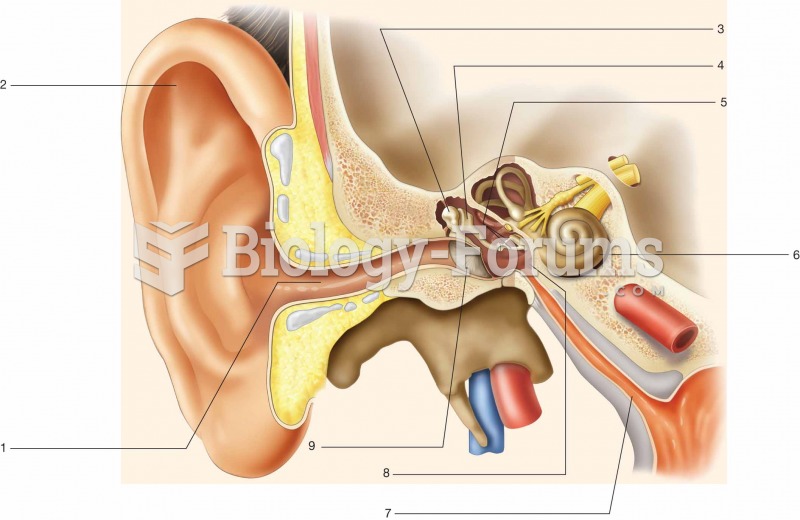 Identify the structures shown below by filling in the blanks.
Identify the structures shown below by filling in the blanks.
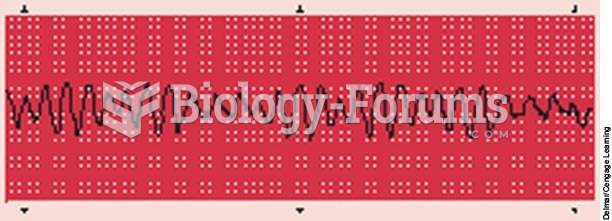 Ventricular fibrillation (VF).
Ventricular fibrillation (VF).
 These illustrations show Ellen Craft, a slave with and without a disguise. She dressed “as a disting
These illustrations show Ellen Craft, a slave with and without a disguise. She dressed “as a disting
 If the thermostat has a jiggle valve, it should be placed toward the top to allow air to escape. If ...
If the thermostat has a jiggle valve, it should be placed toward the top to allow air to escape. If ...
 The U.S. military uses its own marking system to identify explosive hazards (left), chemical hazards ...
The U.S. military uses its own marking system to identify explosive hazards (left), chemical hazards ...