Answer to Question 1
Answer:
Staff Model HMOs
In a Staff HMO, the HMO owns the facility and hires the staff. When a patient comes for a visit, the copayment amount is collected from the patient by the HMO. This money is kept by the HMO and added to premiums to cover their costs of doing business.
The practitioners on staff, whether physicians, nurses, or specialists, are paid a standard salary based on the work they do and the hours they are at work. The amount remains the same regardless of the number of patients they see or the number of procedures they perform.
The HMO covers all costs, including the costs of the facilities, equipment and supplies, and personnel.
In this arrangement, appointments are often made through the HMO, rather than through the provider. This allows the HMO to monitor the number of patients the provider sees and the services performed. If the patient needs additional services, the staff provider will write an order for the services, letting the HMO know that these services are needed.
Since providers are not reimbursed per procedure, there is little benefit to performing or ordering services the patient does not need.
Additionally, if an HMO feels a provider is referring too many patients for additional services, they will limit the number of referrals he may make or may insist on additional documentation to justify the services.
In this model, there are no claims to process since all costs and services are handled by the HMO.
Group Model HMOs
In a Group model HMO, a medical facility or Group bands together to provide services for HMO patients at their own facilities. This is much like the staff model HMO in that the providers receive a salary based on their qualifications and working hours. However, rather than receiving payment directly from the HMO, they receive their salary from the Group. The Group itself receives a capitation amount from the HMO to cover a wide range of services.
If there are any services which the Group is contracted to provide, but cannot supply themselves, they must cover the cost of these services.
If the patient needs services which are not covered by the provider Group, they are referred back to the HMO. The HMO will then provide these services at one of their facilities. These facilities may be either wholly owned by the HMO and thus paid as a staff model, or they may be another Group that has contracted with the HMO to provide all inpatient hospital treatment. If the hospital is a staff arrangement, the HMO covers all costs. If it is a Group arrangement, they receive a capitated amount. Any amount remaining from the premiums after all Groups have been paid their capitated amounts is used to cover the costs of services which they are contractually obligated to cover, but for which there is no provider under contract.
In a Group setup, patients may see different doctors in the Group each time they visit the Group offices. The copayment amount for each visit is collected by the Group and is used to cover their costs.
Rather than building their own facilities, some HMOs are contracting with hospitals to take over a specified number of beds or a wing of an existing hospital. This has come about due to the increased costs of building a new hospital facility and the decreased utilization of hospitals. With HMOs, doctors are encouraged to shorten the length of stay at hospitals. Thus, some hospitals have only 40 to 50 of their beds filled at any given time. Sharing a facility can be a good way to provide an HMO the resources and treatment options needed while at the same time increasing the revenues of the hospital. HMO personnel are usually used to care for patients at these facilities.
Answer to Question 2
Answer: F

 Head rubbing and licking are common social behaviours within a pride
Head rubbing and licking are common social behaviours within a pride
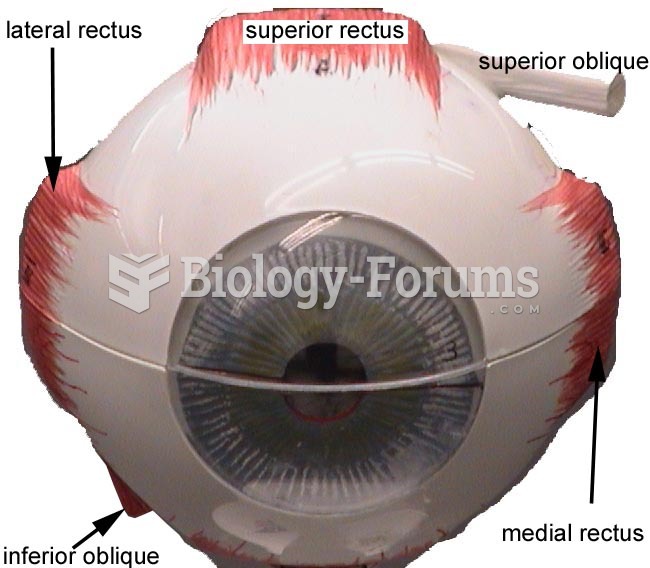 Eye Model
Eye Model
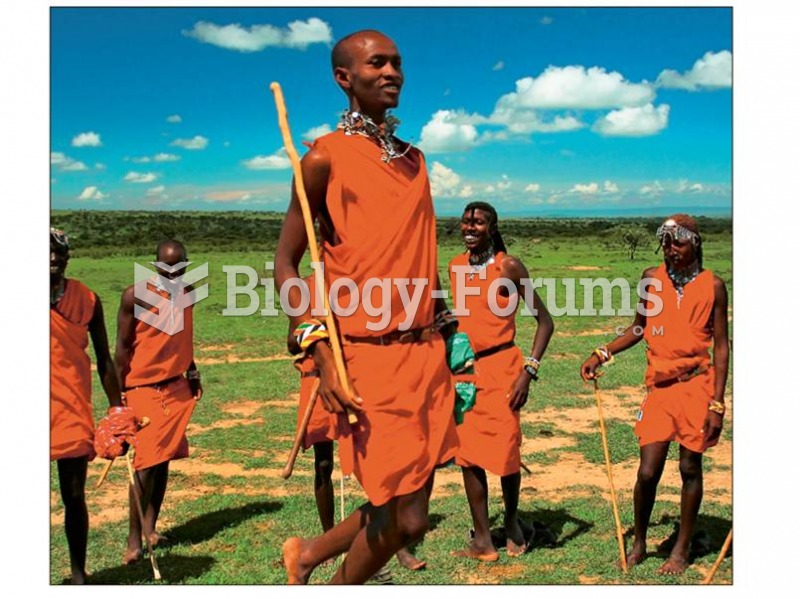 (a) Masai from East Africa have body types adapted to warm climates.
(a) Masai from East Africa have body types adapted to warm climates.
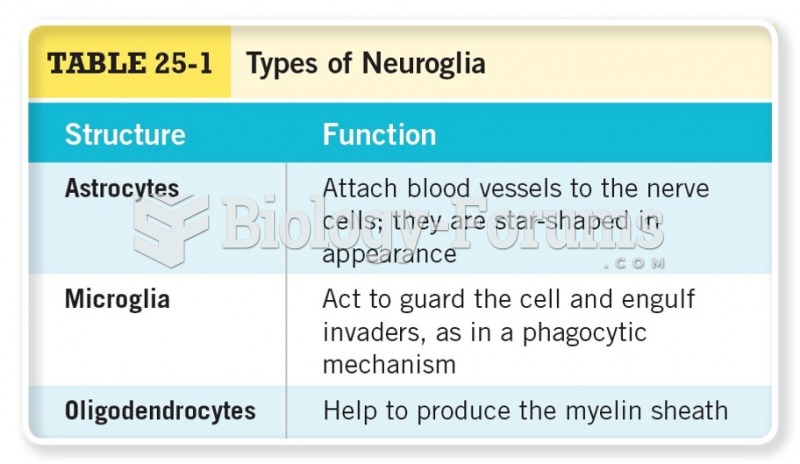 Types of Neuroglia
Types of Neuroglia
 Can you identify the banding patterns predicted by each model after the first round of ...
Can you identify the banding patterns predicted by each model after the first round of ...
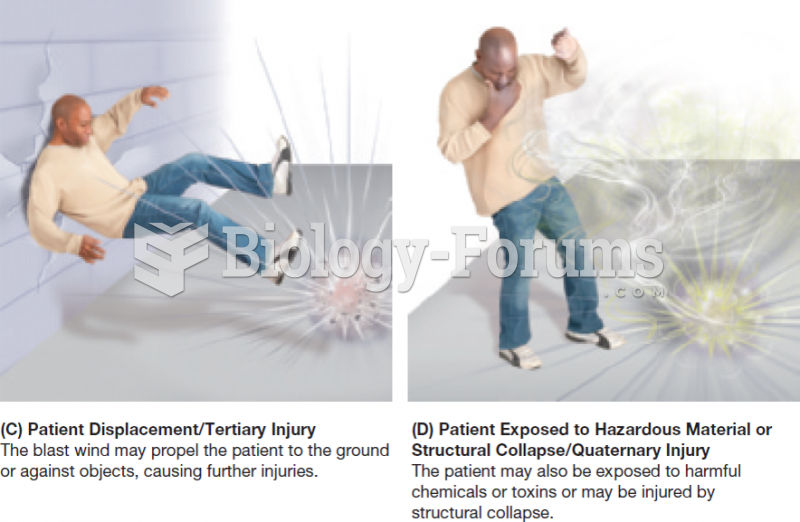 Types of Blast Injuries (Part 2 of 2)
Types of Blast Injuries (Part 2 of 2)