Answer to Question 1
2
Explanation:
1. The medication must be continued for life.
2. The parents should be cautioned to dress the child appropriately to prevent hypothermia.
3. The infant formula is not contraindicated with the prescribed medication.
4. The child will continue to need monitoring and intervention even if growth and development are not affected.
Answer to Question 2
2
Explanation:
1. Although this nursing diagnosis is applicable, pain is a lower priority than is risk for fluid volume deficit.
2. Adequate fluid volume is a critical physiologic need; therefore, this is the highest-priority nursing diagnosis.
3. Although this nursing diagnosis may be applicable, family coping is a lower priority than is risk for fluid volume deficit.
4. Although this nursing diagnosis may be applicable, a knowledge deficit is a psychosocial issue, and therefore a lower priority than is the physiologic need for adequate fluid volume.

 Patients with physical special needs, such as a wheelchair, need to have this documented in their he
Patients with physical special needs, such as a wheelchair, need to have this documented in their he
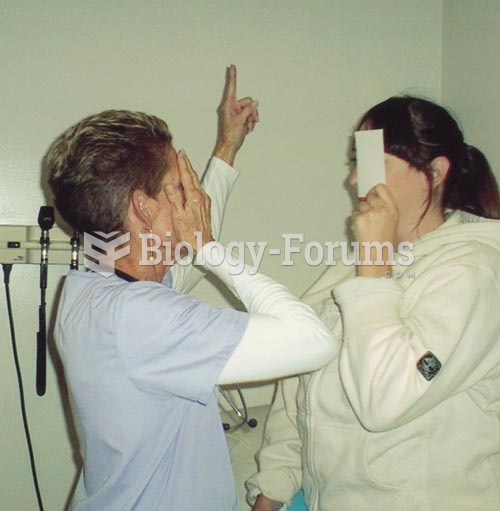 Testing Visual Fields by Confrontation: The nurse and patient should be approximately at an eye to e
Testing Visual Fields by Confrontation: The nurse and patient should be approximately at an eye to e
 The health history can be gathered from many sources
The health history can be gathered from many sources
 Martha Rosler, Gladiators, from the series House Beautiful: Bringing the War Home. 2004
Martha Rosler, Gladiators, from the series House Beautiful: Bringing the War Home. 2004
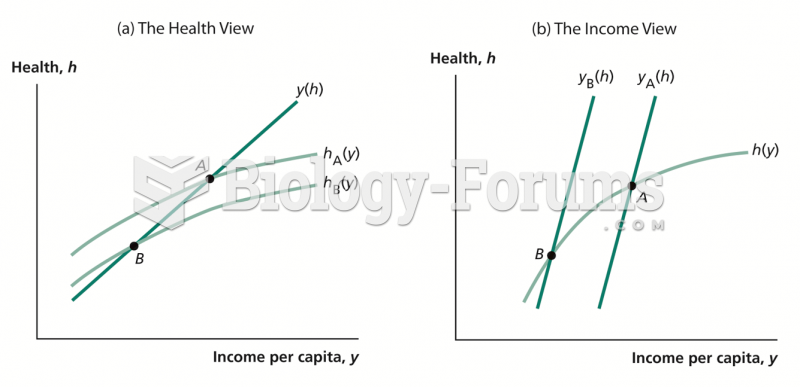 Health and Income per Capita: Two Views
Health and Income per Capita: Two Views
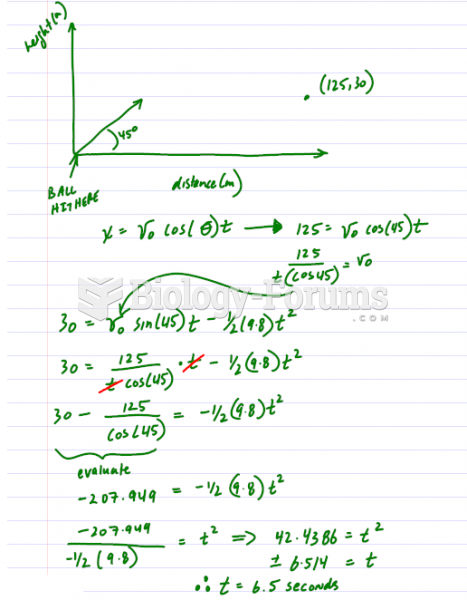 Barry Bonds hits a 125m (450') home run that lands in the stands at an altitude 30m above its ...
Barry Bonds hits a 125m (450') home run that lands in the stands at an altitude 30m above its ...