Answer to Question 1
1
Rationale:
1. The client undergoing manual removal of the placenta will need either IV sedation or general anesthesia. An IV is necessary.
2. Anti-embolism stockings are used after major surgery that leads to immobility, thus increasing the risk of embolism. However, anti-embolism stockings are not needed for this client, because manual removal of the placenta is not major surgery, and does not lead to post-procedure immobility.
3. The client's partner or family member, or a nursery nurse, can feed the infant. The client is at risk for excessive blood loss due to retained placenta, and preparation for manual removal of the placenta is a higher priority at this time.
4. The placenta might be sent to pathology after it is removed, but preparing the client for manual removal of the placenta now is a higher priority.
Answer to Question 2
1
Rationale:
1. Squatting increases the diameter of the pelvic outlet, and might facilitate vaginal birth when cephalopelvic disproportion is a risk.
2. A client with a large fetus and a small pelvis has a higher-than-average chance of needing a cesarean. This client should either be given only clear liquids or be n.p.o. to reduce the risk of aspiration should a cesarean need to be performed.
3. The cervix is normally assessed when the client's labor status appears to have changed, or in order to determine whether cervical change is taking place. The cervix would be assessed more frequently if a client were in the active phase of labor, and cephalopelvic disproportion were a risk. Every eight hours is too far apart.
4. Although it is true that labor with a large fetus and a small pelvis could be prolonged, informing the couple of this fact is a psychosocial intervention. Physiologic interventions are a higher priority.

 A recent study found that female baboons that groom each other are more likely to come to each other
A recent study found that female baboons that groom each other are more likely to come to each other
 Female tule elk
Female tule elk
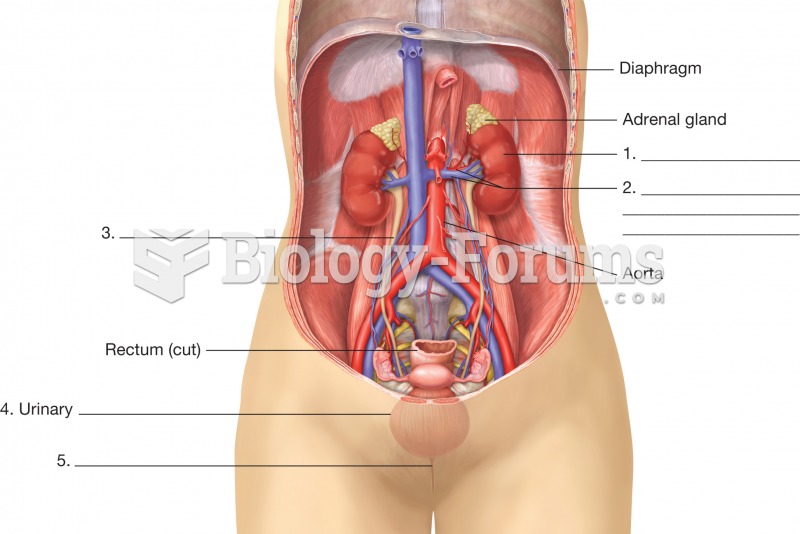 Organs of the urinary system. This illustration is an anterior view of a female with the abdominal w
Organs of the urinary system. This illustration is an anterior view of a female with the abdominal w
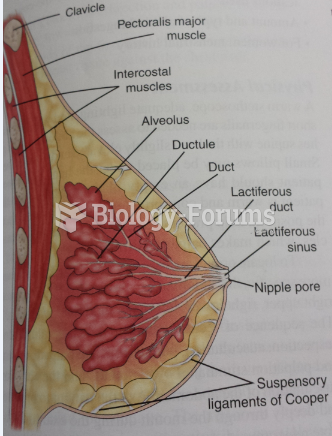 Female Breast
Female Breast
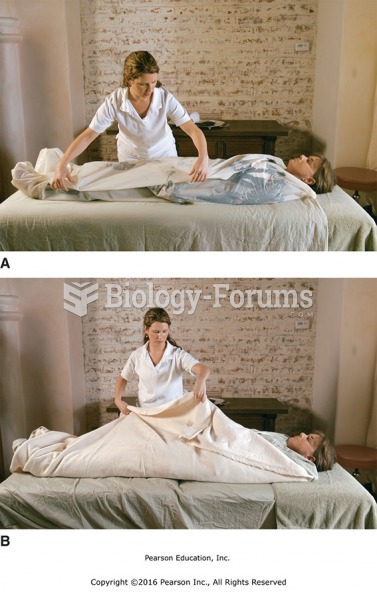 Wrap the client securely with sheets. (A) Lay one side of the sheet over the body. (B) Enclose the ...
Wrap the client securely with sheets. (A) Lay one side of the sheet over the body. (B) Enclose the ...