Answer to Question 1
Kimura studied hemispheric processing of language in people who use sign language rather than speech to communicate. She found that the locations of lesions that would be expected to disrupt speech also disrupt signing. Furthermore, the hemispheric pattern of lesions associated with signing deficits is the same pattern shown with speech deficits. That is, all right-handers with signing deficits show left-hemisphere lesions, as do most left-handers. But some left-handers with signing deficits show right-hemisphere lesions. This finding supports the view that the brain processes both signing and speech similarly in terms of their linguistic function. It refutes the view that signing involves spatial processing or some other nonlinguistic form of cognitive processing.
Answer to Question 2
Malefemale differences in conversational style largely center on differing under- standings of the goals of conversation, according to Tannen. These cultural differences result in contrasting styles of communication. These in turn can lead to misunderstandings and even break-ups as each partner somewhat unsuccessfully tries to understand the other. According to Tannen, men see the world as a hierarchical social order in which the purpose of communication is to negotiate for the upper hand, to preserve independence, and to avoid failure. Each man strives to one-up the other and to win the contest. Women, in contrast, seek to establish a connection between the two participants, to give support and confirmation to others, and to reach consensus through communication.
To reach their conversational goals, women use conversational strategies that minimize differences, establish equity, and avoid any appearances of superiority on the part of one or another conversant. Women also affirm the importance of and the commitment to the relationship. They handle differences of opinion by negotiating to reach a consensus that promotes the connection and ensures that both parties at least feel that their wishes have been considered. They do so even if they are not entirely satisfied with the consensual decision.
Men enjoy connections and rapport. But because men have been raised in a gender culture in which status plays an important role, other goals take precedence in conversations. Men seek to assert their independence from their conversational partners, suggests Tannen. In this way, they clearly indicate their lack of acquiescence to the demands of others, which would indicate lack of power. Men also prefer to inform (thereby indicating the higher status conferred by authority) rather than to consult (indicating subordinate status) with their conversational partners. The male partner in a close relationship thus may end up informing his partner of their plans. In contrast, the female partner expects to be consulted on their plans. When men and women engage in cross-gender communications, their crossed purposes often result in miscommunication because each partner misinterprets the other's intentions.

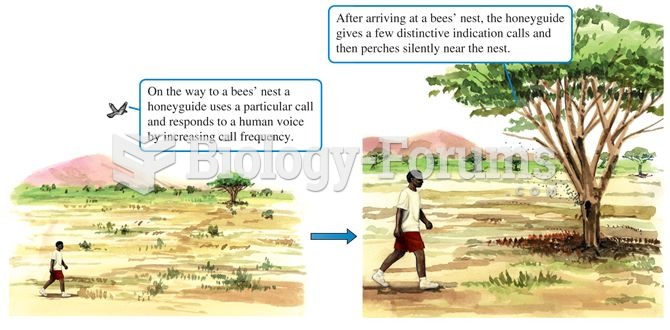 Vocal communication between honeyguides and humans.
Vocal communication between honeyguides and humans.
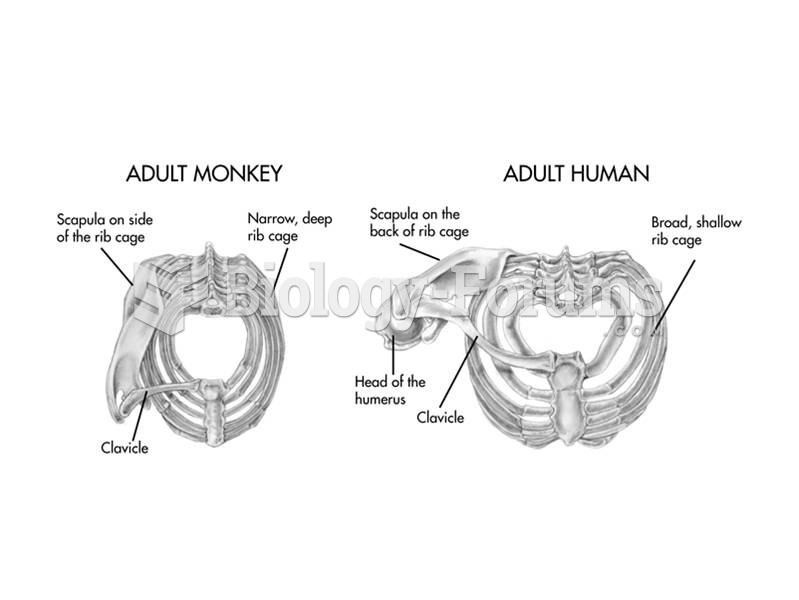 The thorax of apes, including humans, is broad but shallow in contrast to the narrower, deeper chest
The thorax of apes, including humans, is broad but shallow in contrast to the narrower, deeper chest
 Medical Language Communication
Medical Language Communication
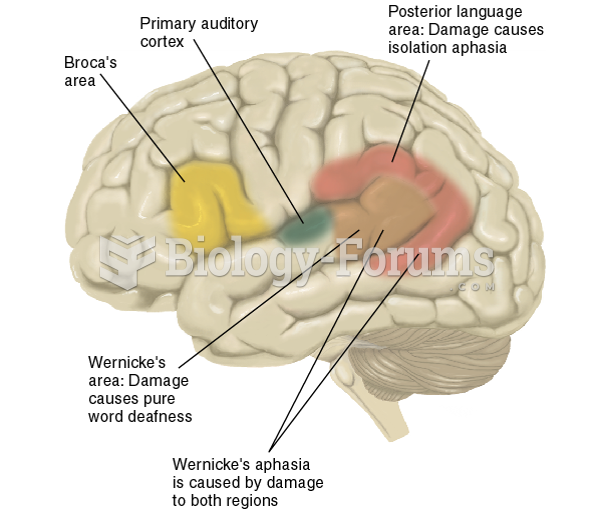 Locations of Broca’s Area, Wernicke’s Area, and Associated Areas Involved in Language Deficits
Locations of Broca’s Area, Wernicke’s Area, and Associated Areas Involved in Language Deficits
 Animals and Language (2 of 2)
Animals and Language (2 of 2)
 Humans are related to Earth’s other organisms
Humans are related to Earth’s other organisms