Answer to Question 1
ANS: C
Nursing interventions and treatments (e.g., medication administration) must be documented. Avoid using generalized, empty phrases such as status unchanged or had good day. Do not document retaliatory or critical comments about a patient, like demanding and argumentative. Family is poor is not critical information to chart.
Answer to Question 2
ANS: C
List actual time of discharge, mode of transportation, and who accompanied the patient for discharge summary information. Clinical decision support systems (CDSSs) are computerized programs used within the health care setting, to aid and support clinical decision making. The knowledge base within a CDSS contains rules and logic statements that link information required for clinical decisions in order to generate tailored recommendations for individual patients that are presented to nurses as alerts, warnings, or other information for consideration. A nurse completes a nursing history form when a patient is admitted to a nursing unit, not when the patient is discharged. SOAP notes are not given to patients who are being discharged. SOAP notes are a type of documentation style.

 The tone of the nurse-patient introduction sets the stage for the patient interview and patient care
The tone of the nurse-patient introduction sets the stage for the patient interview and patient care
 The nurse applies a pulse oximeter sensor on the client’s finger.
The nurse applies a pulse oximeter sensor on the client’s finger.
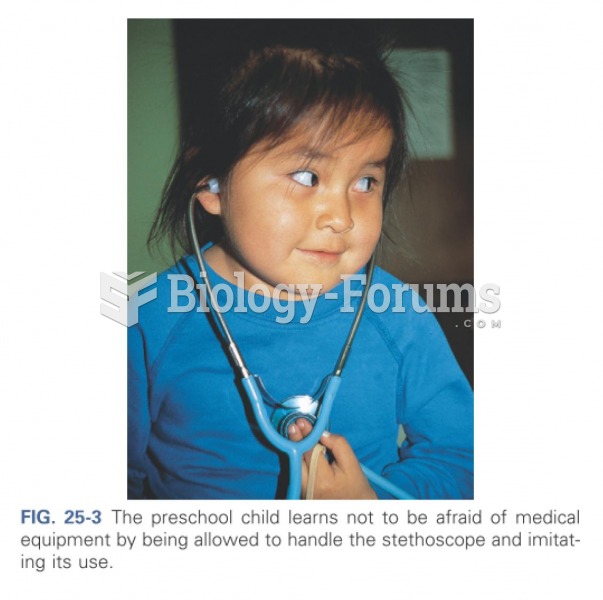 Patient learns to not be afraid
Patient learns to not be afraid
 Instructing a Patient to Use Crutches Correctly
Instructing a Patient to Use Crutches Correctly
 The driver information display on a Chevrolet Impala with a 5.3 liter V-8 equipped with active fuel ...
The driver information display on a Chevrolet Impala with a 5.3 liter V-8 equipped with active fuel ...
 Understanding the Essentials of Critical Care Nursing
Understanding the Essentials of Critical Care Nursing