Answer to Question 1
Ht: 60
Weight: 90, 41 kg
UBW: 110, 50 kg
BMI: 17.6/underweight
UBW: 81.8
This patient is at an increased risk for medical and nutritional complications during the course of her Parkinson's disease because of her recent weight loss and underweight status.
The loss of 18.2 of her bodyweight over a 6 month period (>10) is suggested of severe malnutrition due to chronic illness.
Answer to Question 2
Some level of sodium restriction is necessary in the treatment of heart failure because of the complications associated with severe fluid retention. Sodium in the body attracts fluid, meaning that an excess of sodium from the diet will cause additional fluid retention. Excessive fluid retention causes peripheral edema, ascites, and pulmonary congestion in heart failure patients. The clinical manifestations of fluid overload can increase the patients' energy expenditure (increased work of breathing/respiration rate), while causing eating difficulties (dyspnea, ascites pressing against the stomach). It is essential that these patients control their intake of sodium, which in turn controls their level of fluid retention.
A 2,000 mg sodium diet is a standard initial recommendation.
Adjustments to levels of 1,000 mg or 500 mg may be prescribed depending on an individual patient's medical conditionspecifical ly, fluid and volume states as well as overall oral intake.
These levels of sodium restriction are a challenge to manage outside a hospitalized setting, so it is critical to evaluate the patient's actual PO intake to determine the level of sodium the patient is consuming prior to putting any further modifications in place. However, in malnourished or cachectic patients who have anorexia, caution should be exercised. This is because the first priority in the HF patient is to ensure they are getting enough nutrients to maintain weight and support healing.
Such difficulties include: sodium's high prevalence in Western/processed foods, salt's prominent role in flavor/taste, and salt's high use in foods at restaurants

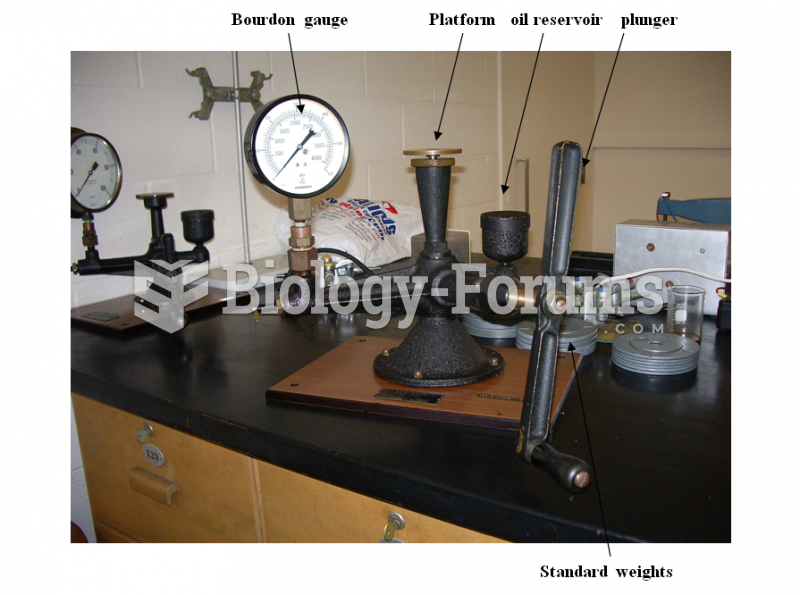 Dead Weight Testers Experiment
Dead Weight Testers Experiment
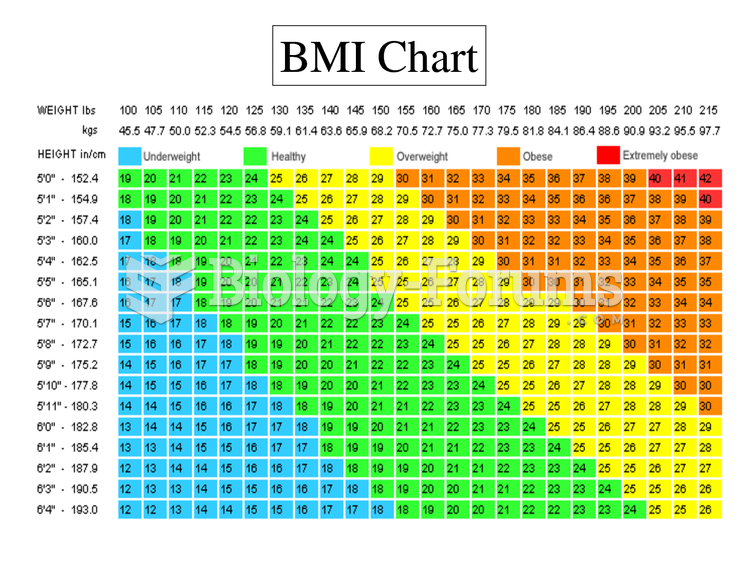 BMI Chart Weight Chart
BMI Chart Weight Chart
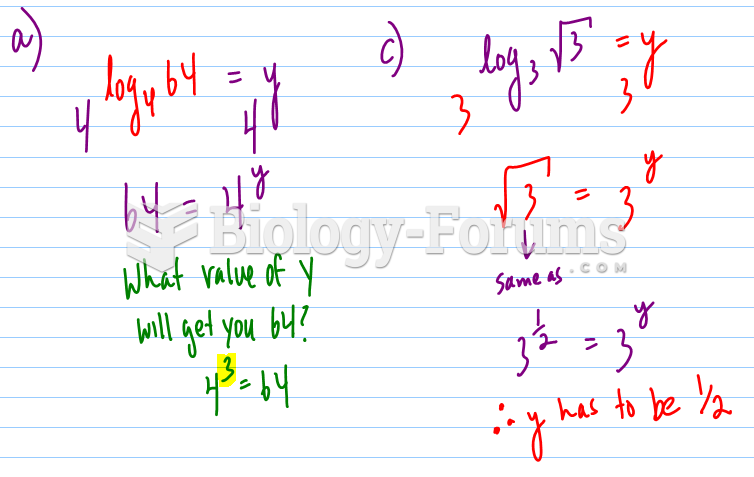 Evaluate each of the following:
Evaluate each of the following:
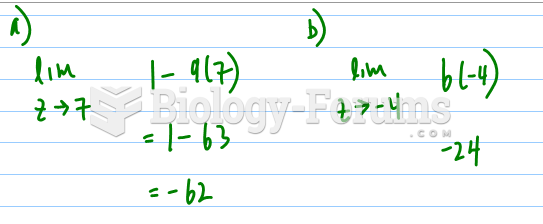 Evaluate the following limits, if they exist - Pt 2
Evaluate the following limits, if they exist - Pt 2
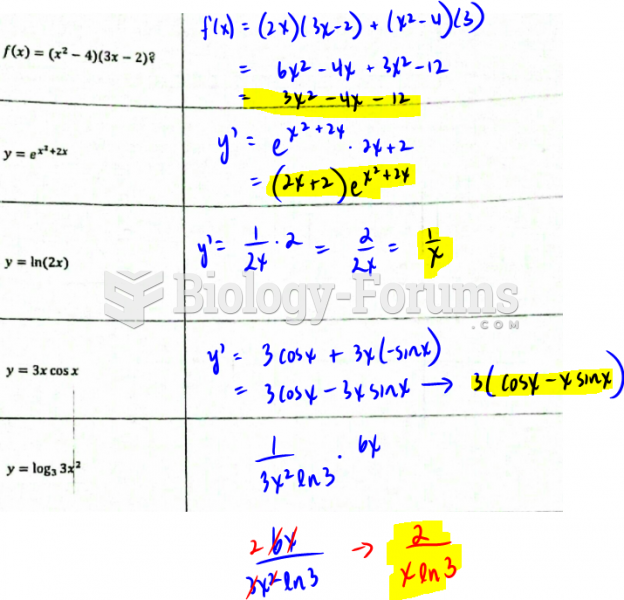 Evaluate the first derivation of the following functions.
Evaluate the first derivation of the following functions.
 For the circuit in Figure 1, assume ideal diodes. The peak inverse voltage is approximately
For the circuit in Figure 1, assume ideal diodes. The peak inverse voltage is approximately