Answer to Question 1
Jugular venous distention
Ascites
2+ pedal edema
Shortness of breath
Increased pulse (110) respirations (24), lower blood pressure (90/70)
Rales
Skin - gray
a) Rales
Due to decreased cardiac output and the resulting low blood pressure present in HF, the RAAS is activated by the kidneys. This system attempts to raise blood pressure by increasing sodium and water retention. Fluid accumulates in the pulmonary vein and backs up into pulmonary circulation, which increases pressure in the pulmonary capillaries. This increased pressure pushes fluid into the lungs, causing pulmonary congestion/edema. The presence of fluid in the lungs can be heard through a stethoscope as rales or crackles as the air tries to move through the fluid with each breath. Because the system lacks the oncotic pressure to pull the fluid back into the capillaries, it continues to accumulate in the lungs, leading to labored breathing and dyspnea. This, in turn, leads to tachypnea, as the patient must breathe more rapidly to get enough oxygen into the lungs.
b) 2+ pedal edema
As the heart enters right-sided HF, it remains unable to pump blood efficiently. The right side of the heart cannot maintain cardiac output, so blood volume decreases. The decrease in renal blood flow again activates the RAAS to increase sodium and water retention, which then causes fluid to back up into the systemic circulation.5 This increased venous pressure in the systemic circulation causes fluid to leak from the capillaries into the third spaces near the ankles and feet (largely due to gravity) leading to pedal edema. Again, the heart is not strong enough and the vessels lack the oncotic pressure needed to pull the fluid back into circulation, so it continues to accumulate, increasing the severity of the edema.
c) Tachycardia
As the failing heart works to increase cardiac output to normal levels, it must beat harder and faster to do so. The release of hormones by the sympathetic nervous system not only cause vasoconstriction and activation of the RAAS, but also increase the heart rate and contractility.
Answer to Question 2
Many different events can lead to the development of congestive heart failure.
Previous myocardial infarction, valve defect, or increased work demand on the heart from other conditions such as hypertension all can damage the heart.
This damage results in a decreased ability of the heart to pump adequately.
When there is reduced blood flow to tissues, the body compensates in several ways.
The kidney responds to decreased blood flow by secreting renin and aldosterone, causing vasoconstriction and an increase in blood volume.
The heart then has to work even harder to handle the increased blood volume.
Over time, the heart enlarges (cardiomegaly) with its attempt to handle the increased workload.
Cardiac output and stroke volume decrease.
Compensation mechanisms do work for a time but eventually the heart muscle weakens.
Dr. Maney's medical history is consistent with the typical pathophysiology of heart failure. She has a long history of coronary artery disease, hypertension, and mitral valve disorder. She also experienced a myocardial infarction. Her previous medical diagnoses are all indicative of damage to the heart muscle, which is the first step in the progression of heart failure.

 The patient and his family meet with the nurse to discuss progress on the patient care plan.
The patient and his family meet with the nurse to discuss progress on the patient care plan.
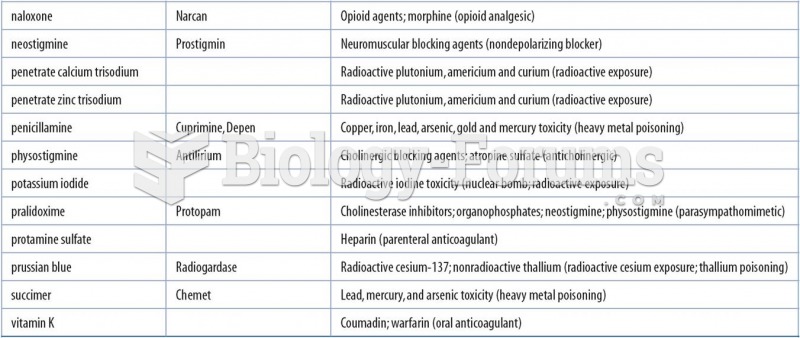 Examples of Specific Antidotes for Overdosed Substances or Toxins
Examples of Specific Antidotes for Overdosed Substances or Toxins
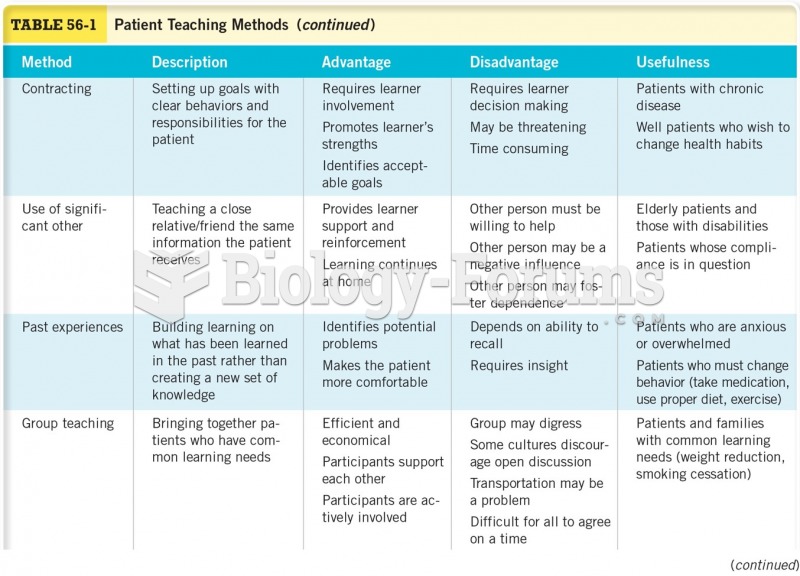 Patient Teaching Methods Cont.
Patient Teaching Methods Cont.
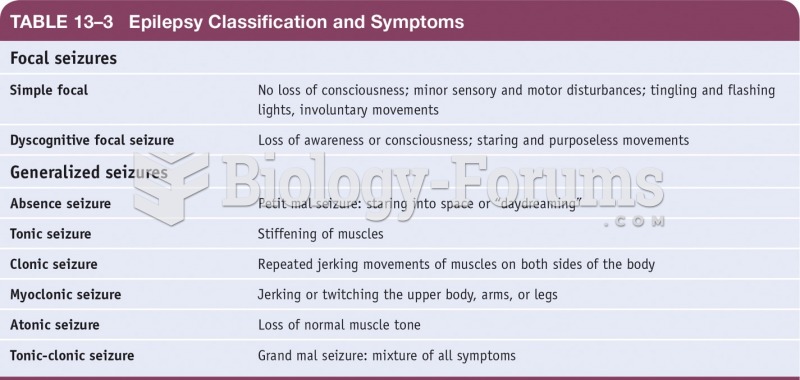 Epilepsy Classifications and Symptoms
Epilepsy Classifications and Symptoms
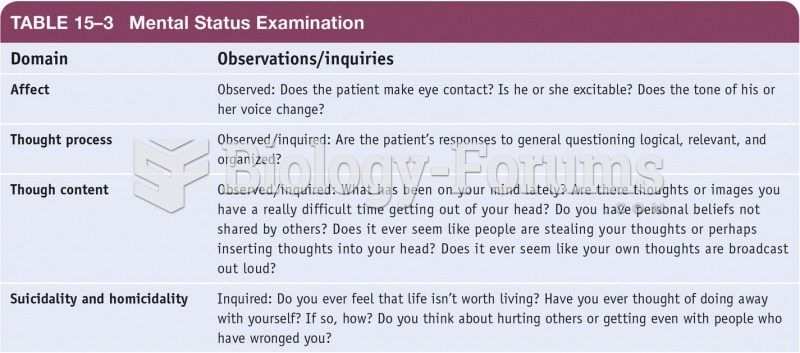 Mental Status Examination
Mental Status Examination
 The ChIPSeq method screens for specific transcription factor binding sites across a whole genome
The ChIPSeq method screens for specific transcription factor binding sites across a whole genome