You are a public health nurse working at a county immunization and tuberculosis (TB) clinic.
B.A. is a 51-year-old woman who wishes to obtain a food handler's license and is required to show proof of a negative
Mantoux (purified protein derivative PPD) test result before being hired. She came to your clinic 2 days ago to undergo a PPD test for TB. She has returned to have you evaluate her reaction.
What is TB, and what microorganism causes it?
What is the route of transmission for TB?
Question 2
You are in the middle of your shift in the coronary care unit (CCU) of a large urban medical center. Your new admission, C.B., a 47-year-old woman, was just flown to your institution from a small rural community more than 100 miles away.
She had a STEMI (ST segment elevation myocardial infarction) last evening. Her current vital signs (VS) are 100/60, 86, 14. After you make C.B. comfortable, you receive
this report from the flight nurse: C.B. is a full-time homemaker with four children. She has had episodes
of 'chest tightness' with exertion for the past year, but this is her first known MI. She has a history of
hyperlipidemia and has smoked one pack of cigarettes daily for 30 years. Surgical history consists of total
abdominal hysterectomy 10 years ago after the birth of her last child. She has no other known medical
problems. Yesterday at 8 pm, she began to have severe substernal chest pain that referred into her neck
and down both arms. She rated the pain as 9 or 10 on a 0-to-10 scale. She thought it was severe indigestion
and began taking Maalox with no relief. Her husband then took her to the local emergency department,
where a 12-lead electrocardiogram (ECG) showed hyperacute ST elevation in the inferior leads II,
III, aVF and V5 to V6. Before tissue plasminogen activator could be given, she went into ventricular fibrillation
(V-fib). CPR was started and when the code team arrived, she was successfully defibrillated after
two shocks. She then was started on nitroglycerin (NTG), heparin, and amiodarone drips. She was given
IV metoprolol and aspirin 325 mg to chew and swallow. This morning her systolic pressure dropped into
the 80s, and she was placed on a low-dose norepinephrine drip and urgently flown to your institution for
coronary angiography and possible percutaneous transluminal coronary angioplasty. Currently, she has
amiodarone infusing at 1 mg/min, heparin at 1200 units/hr, and norepinephrine at 0.5 mcg/kg/min. The
NTG has been stopped because of low blood pressure. Laboratory work that was done yesterday showed
Na 145 mEq/L, K 3.6 mEq/L, HCO3 19 mEq/L, BUN 9 mg/dL, creatinine 0.8 mg/dL, WBC 14,500/mm3, Hct
44.3, and Hgb 14.5 g/dL.
Because the 12-lead ECG can tell you the location of the infarction, evaluate the leads that
showed ST elevation. What areas of C.B.'s heart have been damaged?
Given the diagnosis of acute myocardial infarction (MI), what other laboratory results are
you going to look at?
Indicate the expected outcome for C.B. associated with each medication she is receiving. For
each of the drugs listed, state the purpose.
a. Intravenous (IV) nitroglycerin (NTG)
b. IV heparin
c. IV amiodarone
d. IV metoprolol
e. Aspirin, chewed and swallowed
f. IV norepinephrine
Laboratory Test Results
Creatine Phosphokinase (CK) Levels
On ED admission 95 units/L
4 hours 1931 units/L
8 hours 4175 units/L
CK-MB Isoenzymes
On ED admission 5
4 hours 79
8 hours 216
LDL 160 mg/dL
PT 11.9 sec
INR 1.02
aPTT (before heparin) 26.9 sec
Mg 2.2 mg/dL
K 3.3 mEq/L
You review the lab work on her chart. For each laboratory value listed previously, interpret the result, and evaluate the meaning for C.B.
List at least two complications C.B. is at risk for at this time and the assessments that are
needed to identify these risks.
You note that C.B.'s Spo2 on oxygen (O2) at 6 L/min by nasal cannula is 92. How do you interpret this result?
What can be done to promote her oxygenation at this time?

 A nurse shows empathy to a client.
A nurse shows empathy to a client.
 Large water tank, possibly a public or ritual bathing area, from Mohenjo-daro, Indus Valley ...
Large water tank, possibly a public or ritual bathing area, from Mohenjo-daro, Indus Valley ...
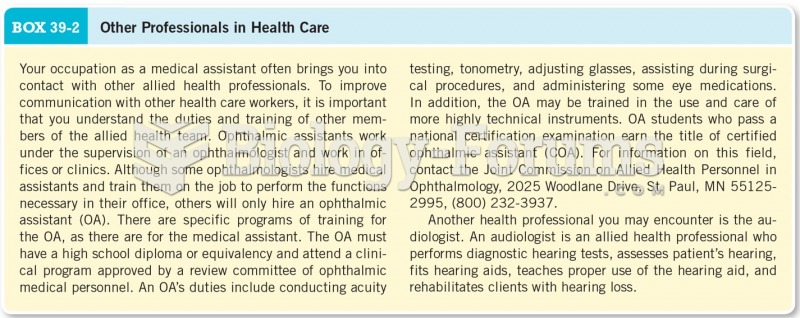 Other Professionals in Health Care
Other Professionals in Health Care
 Cultural Diversity in Health and Illness (9th Edition)
Cultural Diversity in Health and Illness (9th Edition)
 Homework Clinic Logo
Homework Clinic Logo
 health studies homework help
health studies homework help