After assessing K.Z., the physician admits him with a diagnosis of CAD and HF for coronary artery bypass graft (CABG) surgery.
Significant laboratory results drawn at this time are Hct 25.3, Hgb 8.8 g/dL, BUN
33 mg/dL, and creatinine 3.1 mg/dL. K.Z. is given furosemide (Lasix) and 2 units of packed red blood cells
(PRBCs).
Review K.Z.'s health history. Can you identify a probable explanation for his chronic renal
insufficiency and anemia?
Why is he receiving 2 units of PRBCs? What is the purpose of the furosemide?
Question 2
Several hours later, K.Z. returns from his catheterization.
The catheterization report shows 90 occlusion
of the proximal left anterior descending (LAD) coronary artery, 90 occlusion of the distal LAD, 70 to
80 occlusion of the distal right coronary artery (RCA), an old apical infarct, and an ejection fraction (EF)
of 37. About an hour after the procedure is finished, you perform a brief physical assessment and note
a grade III/VI systolic ejection murmur at the cardiac apex, crackles bilaterally in the lung bases, and trace pitting edema of his feet and ankles. Except for the soft systolic murmur, these findings were not present before the catheterization.
What is your evaluation of the catheterization results?
Explain the significance of having an EF of 37.
What problem do the changes in assessment findings suggest to you? What led you to your conclusion?
List five actions you should take as a result of your evaluation of the assessment, and state
your rationales.

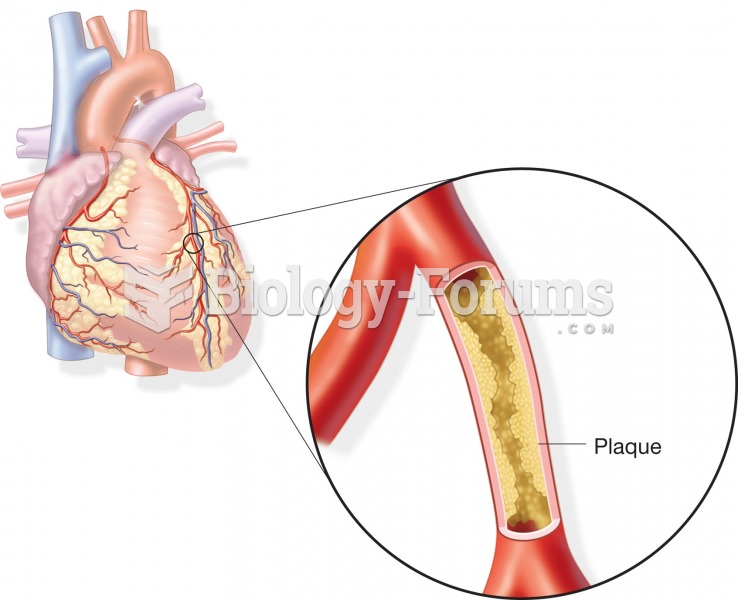 Formation of an atherosclerotic plaque within a coronary artery; may lead to coronary artery disease
Formation of an atherosclerotic plaque within a coronary artery; may lead to coronary artery disease
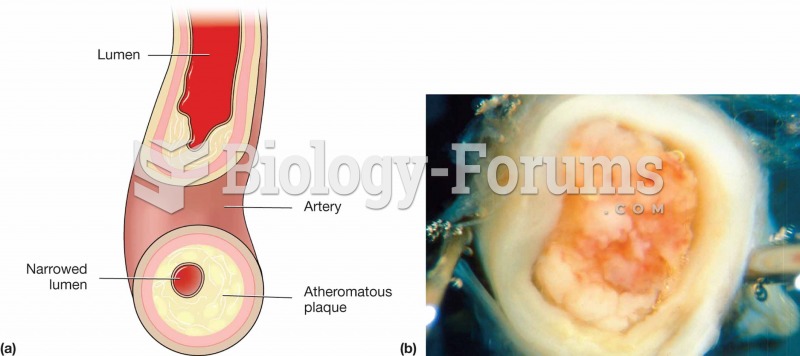
 Atherosclerotic artery.
Atherosclerotic artery.
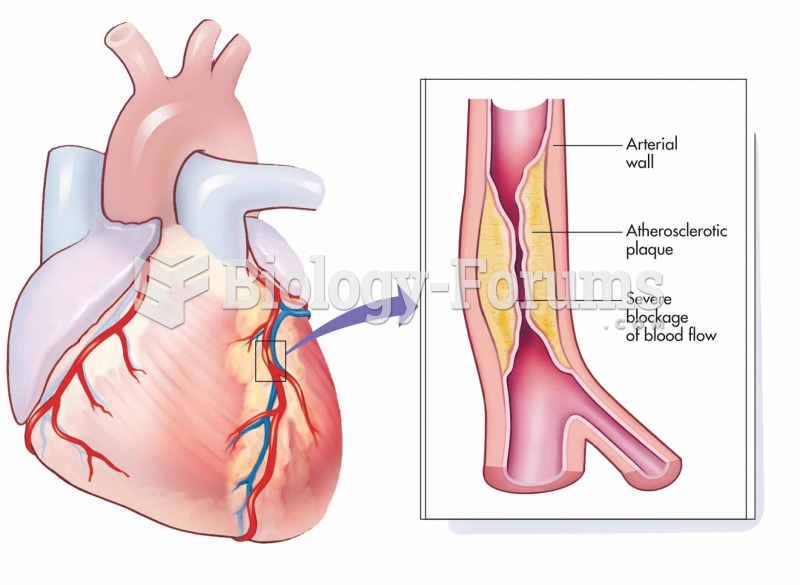
 Severe atherosclerotic plaque in an artery.
Severe atherosclerotic plaque in an artery.
 Assessing Accomodation
Assessing Accomodation
 The physician and medical assistant will often work together to choose appropriate educational ...
The physician and medical assistant will often work together to choose appropriate educational ...
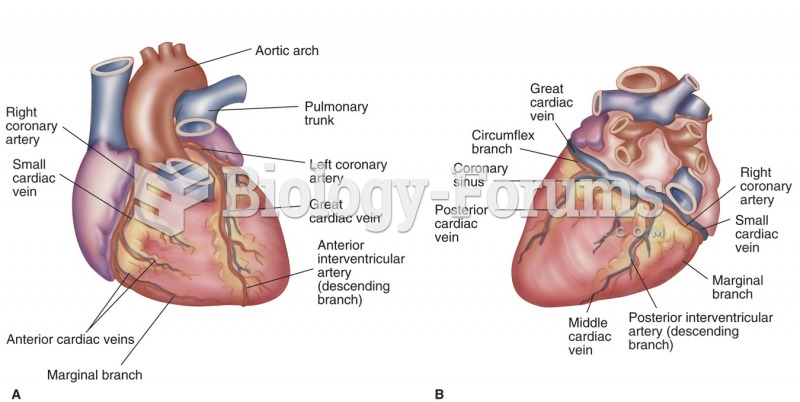 Coronary arteries and major vessels (A) anterior (B) posterior.
Coronary arteries and major vessels (A) anterior (B) posterior.