Answer to Question 1
ANS: A
Anemia is not a disease unto itself but a sign of an underlying disorder, which is common among pregnant women. A hemoglobin less than 11 g/dl in either the first or third trimester or less than 10.5 g/dL in the second trimester is considered anemia (Arnett, Greenspoon, & Roman, 2013). Anemia during pregnancy is associated with high-output CHF, premature delivery, low birth weight, and fetal demise. The etiology of the anemia can be classified according to the size and color of the red blood cells (RBCs) (Table 19.5). The anemias most often diagnosed during pregnancy are folic-acid and iron-deficiency anemia (IDA). The principle etiologies for these anemias are inadequate nutrition, especially among women in lower socioeconomic groups, and the increased body requirements of pregnancy. If IDA is suspected on the basis of a CBC (low hemoglobin and low RBC indices), iron studies should be attained. These iron studies will generally reveal a low serum iron level, decreased serum ferritin, increased total iron-binding capacity, and decreased transferrin saturation percentage (Arnett, Greenspoon, & Roman, 2013). Folate is needed for normal DNA production, but the body stores of folate are limited to a 3-month reserve and may be depleted during high rates of cell turnover, such as during pregnancy. A folate and vitamin B12 level should be checked if the CBC suggests that a macrocytic anemia (low hemoglobin level and an MCV of greater than 100) is the cause. An anemic woman may complain of fatigue and dyspnea on exertion. Common findings include skin pallor, tachycardia, grade II/VI systolic heart murmur, and increased respiratory rate. The CBC will indicate potential causes (see Table 19.5) and guide selection of additional diagnostic studies, such as iron panel, folate level, sickle-cell screen or hemoglobin electrophoresis, and liver function tests. Differential diagnoses include iron deficiency, folate deficiency, vitamin B12 deficiency, sickle cell trait/anemia, and thalassemia.
Answer to Question 2
ANS: A
A 30 to 50 increase in cardiac output occurs during pregnancy (Sakornbut, 2008b). This increase begins as early as 10 weeks of gestation and peaks at 20 to 24 weeks. A 40 to 50 increase in blood volume results in an increased venous pressure below the level of the uterus. This increased pressure can result in varicosities in the legs and perineum (hemorrhoids), especially when the pregnant woman is in an upright position, such as with prolonged sitting or standing. An enlarging uterus compresses the vena cava or pelvic and lower extremity veins, leading to venous pooling, which can result in edema, hypotension, dizziness, or even syncope. In order to lessen these complications, the pregnant woman should be instructed not to lie in a supine or recumbent position, but rather in a left lateral tilt.

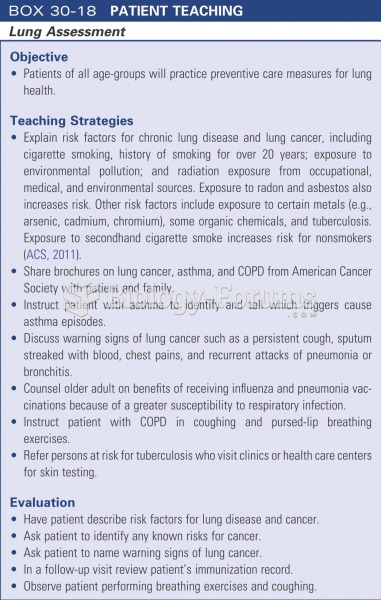 Patient teaching: lung assessment
Patient teaching: lung assessment
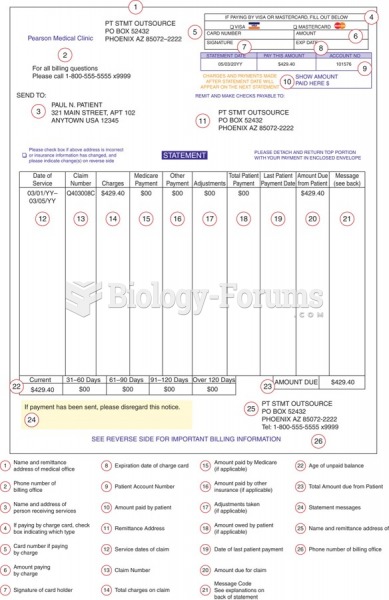 Example of a patient statement.
Example of a patient statement.
 The physician will begin visual inspection of the patient immediately upon entering the examination ...
The physician will begin visual inspection of the patient immediately upon entering the examination ...
 Medical assistant interviewing a patient.
Medical assistant interviewing a patient.
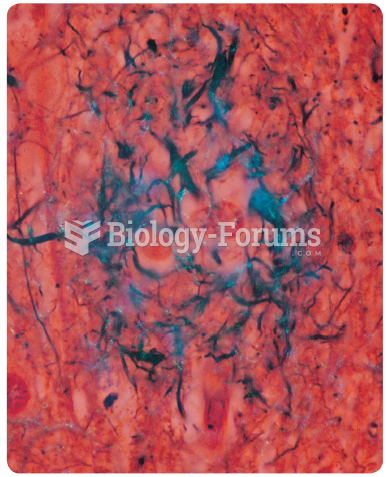 Amyloid plaques (stained blue) in the brain of a deceased patient who had Alzheimer’s disease.
Amyloid plaques (stained blue) in the brain of a deceased patient who had Alzheimer’s disease.
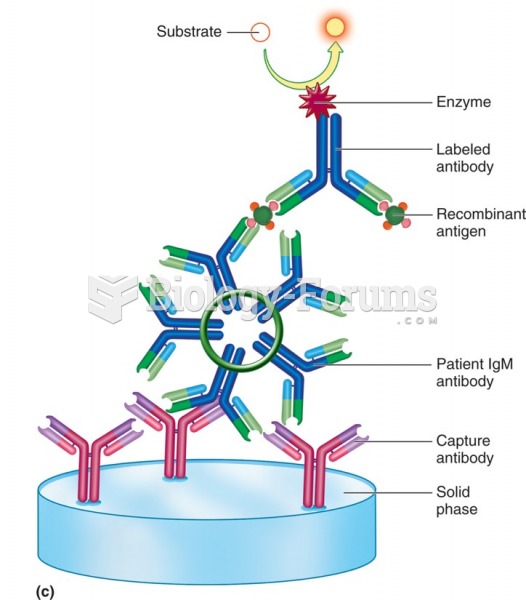 Sandwich or capture enzyme immunoassay for patient IgM (double capture: IgM capture, Ag capture).
Sandwich or capture enzyme immunoassay for patient IgM (double capture: IgM capture, Ag capture).