Answer to Question 1
ANS: B
The menstrual history includes any episodes of amenorrhea, menorrhagia (excessive bleeding at the time of the menstrual cycle), metrorrhagia (bleeding at irregular noncyclic intervals), dysmenorrhea, and postmenopausal bleeding. Amenorrhea has many causes, including pregnancy; anorexia nervosa; excessive exercise; low body fat; and disorders or tumors of the hypothalamus, pituitary gland, ovary, uterus, and thyroid gland. Menorrhagia is most commonly caused by uterine fibroids, but hematologic disorders should be considered. Metrorrhagia can be caused by anovulation, intrauterine devices (IUDs), and ovarian and uterine tumors.
Answer to Question 2
ANS: D
Supplementation with testosterone or with testosterone-like substances can result in decreased endogenous testosterone as well as LH, hypogonadotropic hypogonadism, and suppressed spermatogenesis. Hypogonadism induced by exogenous steroid use is usually temporary, and endogenous hormone production and spermatogenesis rebound after approximately 4 months. The patient may complain of increased or decreased libido and possible ED. There may be some noticeable testicular atrophy on examination. Semen analysis will show oligospermia or azoospermia, and total testosterone will be above the normal range (or supraphysiologic with anabolic use).

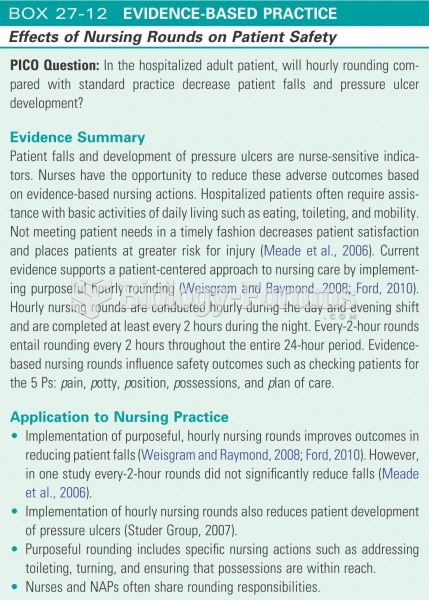 Effects of nursing rounds on patient safety
Effects of nursing rounds on patient safety
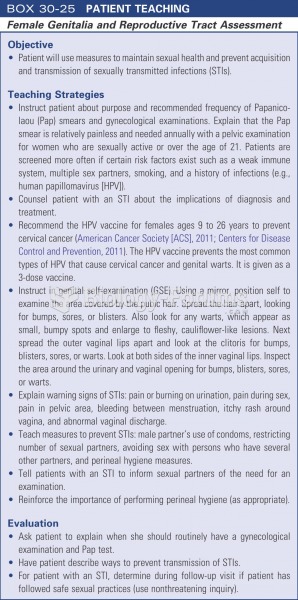 Patient teaching: female genetalia and reproductive tract assessment
Patient teaching: female genetalia and reproductive tract assessment
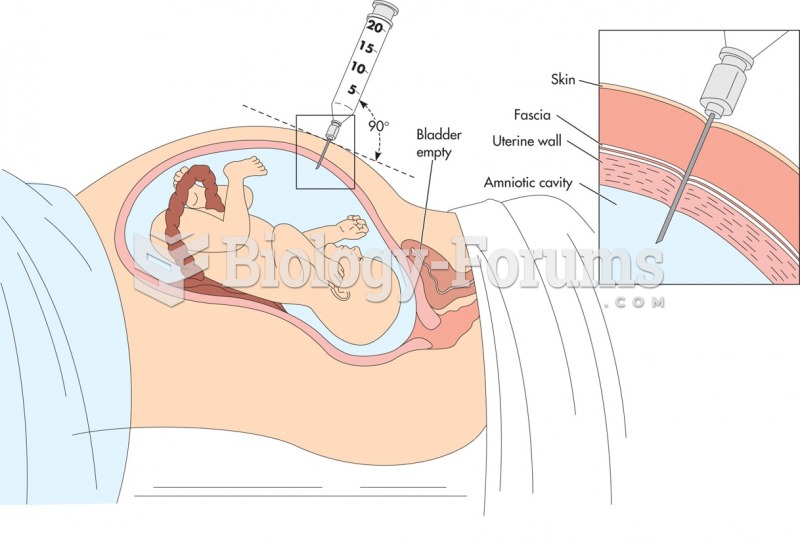 Amniocentesis. The patient is examined with ultrasound to determine the placental site and to locate ...
Amniocentesis. The patient is examined with ultrasound to determine the placental site and to locate ...
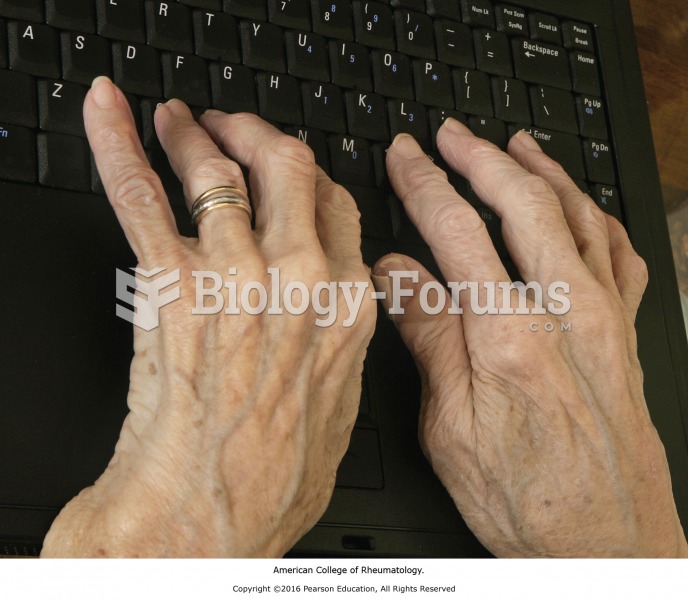 Patient with rheumatoid arthritis.
Patient with rheumatoid arthritis.
 Oral pseudo membraneous candidiasis in a patient with AIDS.
Oral pseudo membraneous candidiasis in a patient with AIDS.
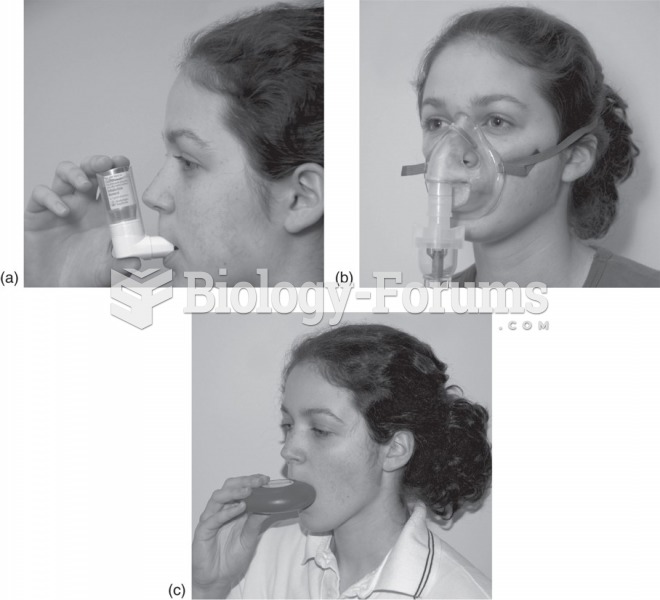 Inhalers used to deliver asthmatic drugs: (a) Metered-dose inhaler. The patient times the inhalation ...
Inhalers used to deliver asthmatic drugs: (a) Metered-dose inhaler. The patient times the inhalation ...