Answer to Question 1
Correct Answer: D
Hyperglycemia causes serum hyperosmolality, drawing water from the intracellular spaces into the general circulation. The increased blood volume increases renal blood flow, and the hyperglycemia acts as an osmotic diuretic. The resulting osmotic diuresis increases urine output. This condition is called polyuria. When the blood glucose level exceeds the renal threshold for glucose usually about 180 mg/dL glucose is excreted in the urine, a condition called glucosuria. The decrease in intracellular volume and the increased urinary output cause dehydration. The mouth becomes dry and thirst sensors are activated, causing the person to drink increased amounts of fluid (polydipsia). A blood glucose level of 60 mg/dL is hypoglycemia. Polyuria is not a manifestation of hypoglycemia. A blood glucose level of 110 mg/dL is considered as being a normal blood glucose level. Polyuria is not a manifestation of a normal blood glucose level. A blood glucose level of 125 mg/dL is consistent with prediabetes. Polyuria is not a manifestation of prediabetes.
Answer to Question 2
Correct Answer: 1, 2
If blood glucose falls, glucagon is released to raise hepatic glucose output, raising glucose levels. Epinephrine, growth hormone, thyroxine, and glucocorticoids (often referred to as glucose counterregulatory hormones) also stimulate an increase in glucose in times of hypoglycemia, stress, growth, or increased metabolic demand. Insulin is not released as a counterregulatory hormone. Thyroxine and glucocorticoids levels would increase with hypoglycemia.

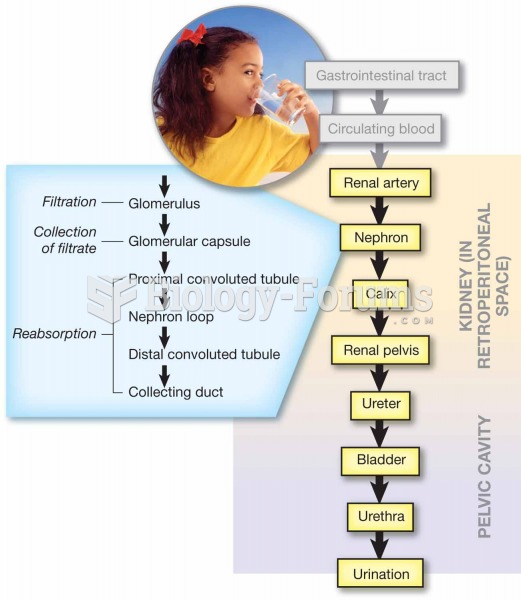 Pathway of urine production and elimination.
Pathway of urine production and elimination.
 Patient teaching: female genetalia and reproductive tract assessment
Patient teaching: female genetalia and reproductive tract assessment
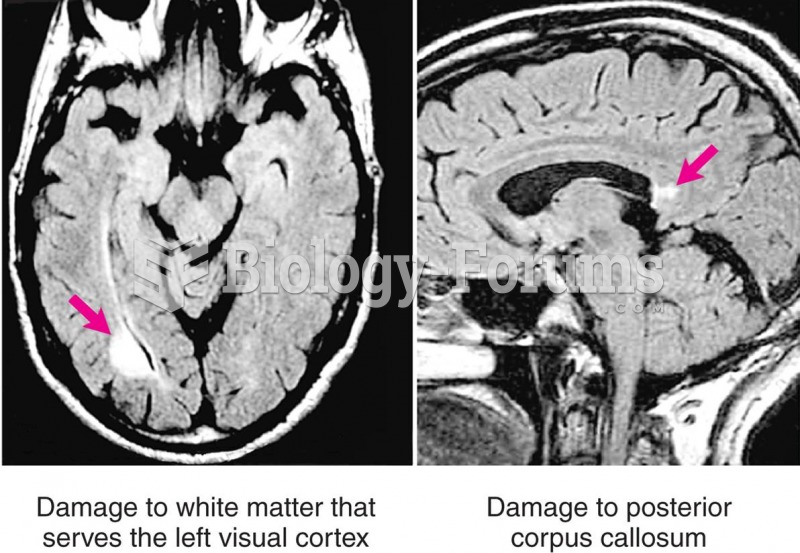 Pure Alexia in a Patient with Multiple Sclerosis
Pure Alexia in a Patient with Multiple Sclerosis
 Oral pseudo membraneous candidiasis in a patient with AIDS.
Oral pseudo membraneous candidiasis in a patient with AIDS.
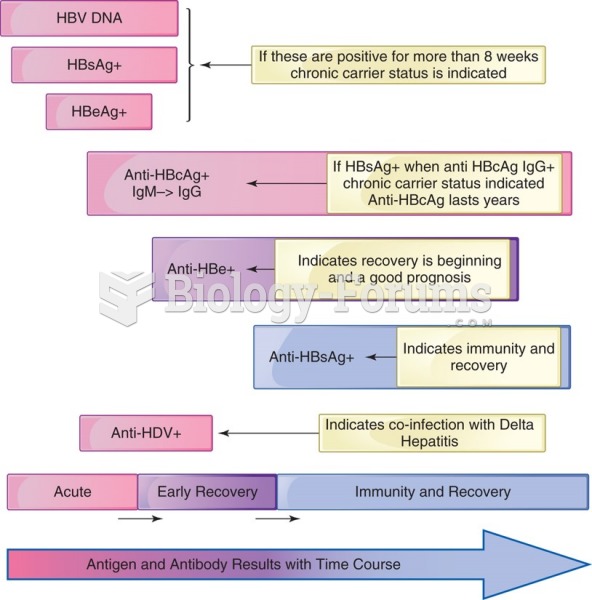 Hepatitis B antigens and antibody in an acutely infected patient with recovery. Note the indicators ...
Hepatitis B antigens and antibody in an acutely infected patient with recovery. Note the indicators ...