Answer to Question 1
Answer: B, D, E
When performing a suicide assessment, the nurse should always use direct, not indirect, questioning. The nurse should ask if the client has any thought of suicide and assess the lethality of the suicide plan, if one exists, and whether or not the client will act on these thoughts. Asking about suicide will not plant the idea in the client's mind.
Answer to Question 2
Answer: B, C
Evaluation of care is based on the family's progress toward goals and outcomes mutually determined by the family and nurse. Examples of achieved outcomes include the following: family members demonstrate more frequent engagement in activities that involve the entire family unit, each family member is up to date with all vaccinations, and individual family members report a decrease in or cessation of behaviors associated with adverse health conditions and disease. Eating donuts for breakfast could indicate poor nutrition. Squinting when reading indicates the need for a vision assessment. And not washing hands before eating could lead to the ingestion of a microorganism that could cause disease.

 Tongue Assessment
Tongue Assessment
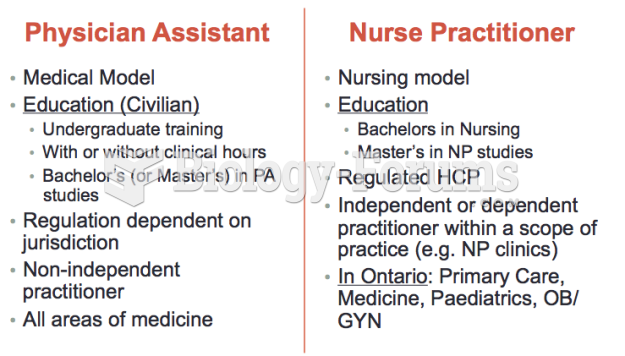 Differences between a Nurse Practitioner
Differences between a Nurse Practitioner
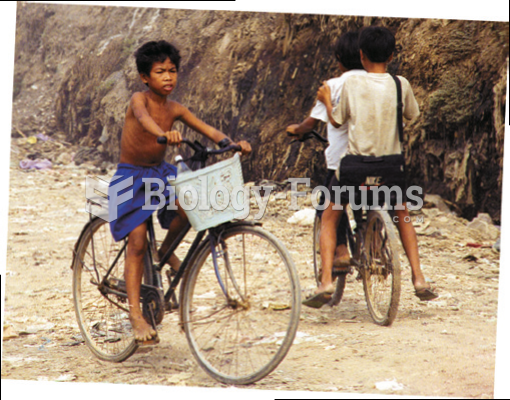 Working and Living and Playing in the City Dump of Phnom Penh, Cambodia
Working and Living and Playing in the City Dump of Phnom Penh, Cambodia
 A funnel helps in hearing if the electric fuel pump inside the gas tank is working.
A funnel helps in hearing if the electric fuel pump inside the gas tank is working.
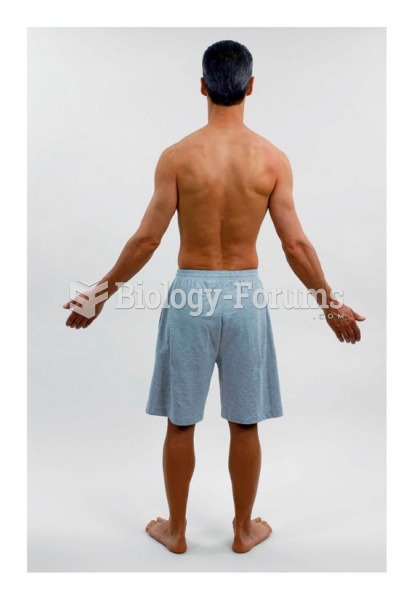 Survey and posture of client: Lateral view
Survey and posture of client: Lateral view
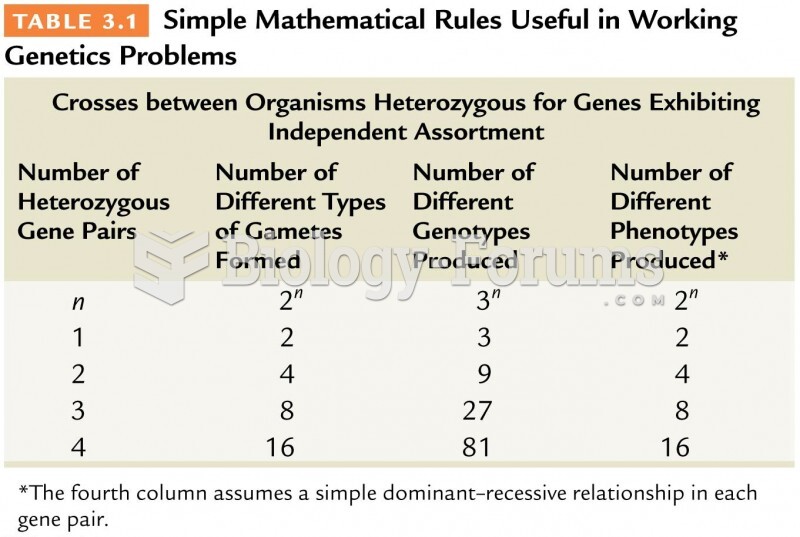 Simple Mathematical Rules Useful in Working Genetics Problems
Simple Mathematical Rules Useful in Working Genetics Problems