Answer to Question 1
Correct Answer: 3
For the initial pulse assessment, the nurse may count the beats for 30 seconds and multiply by 2. It is not necessary for the nurse to count the pulse for 2 minutes, as heart rate is expressed in beats per minute. With any irregular pulse, the rate needs to be counted for 1 full minute Counting for 15 seconds and multiplying by 4 may not yield an accurate result, and therefore should not be used in assessing the rate.
Answer to Question 2
Correct Answer: 4
Pain is a subjective experience, and the response is unique to each individual. The factors that impact the response are numerous and include age, sex, culture, and developmental level, as well as previous experience with pain and health status. Vital signs are only a portion of the pain assessment. The nurse must consider many factors since pain is an individual experience and no two people experience pain in the same way. A patient's level of pain cannot be determined by his physiologic response only. Pain is unique to each person and may be experienced differently by clients with the same diagnosis. Vital signs can be indicators of pain. In the early stages of acute pain, the sympathetic nervous system is stimulated, causing increases in blood pressure, pulse, and respiratory rates.

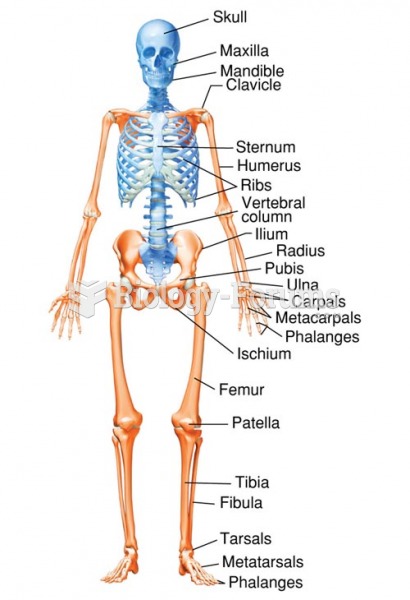 Adult Skeleton: Anterior View
Adult Skeleton: Anterior View
 Carotid pulse.
Carotid pulse.
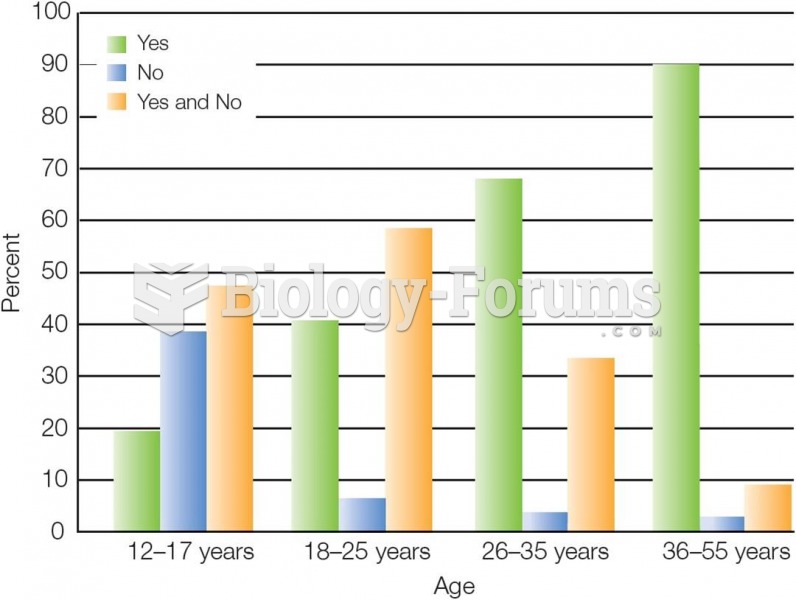 Emerging adults often feel adult in some ways but not others.
Emerging adults often feel adult in some ways but not others.
 Performing Venipuncture Using the Vacutainer Method
Performing Venipuncture Using the Vacutainer Method
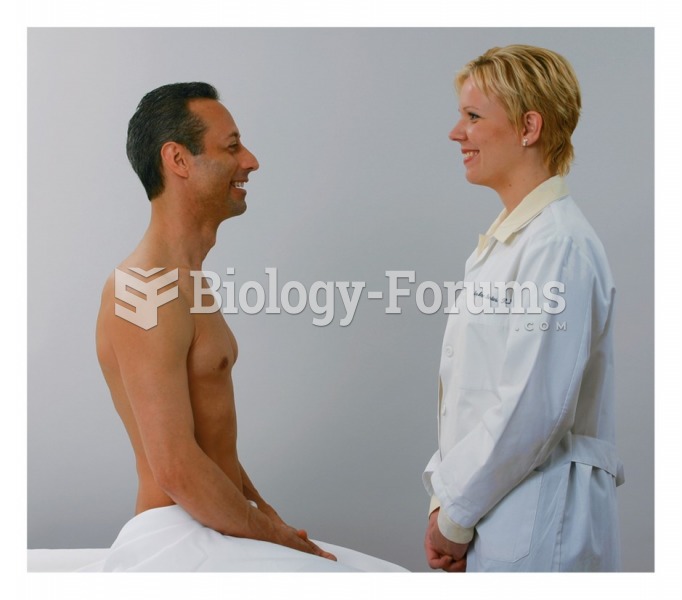 The nurse begins the general survey
The nurse begins the general survey
 Palpating the radial pulse
Palpating the radial pulse