Patient is seen at the ED complaining of an intense right-sided headache. Physical exam showed drooping of the right eyelid, tearing in that eye only, and rhinorrhea right nostril only. There was miosis in the right pupil. The patient stated the headache started very suddenly, qualifying it with, They all do. He described the pain as drilling and was mostly located around the periorbital area. He said, You may as well stick a hot poker in my eye. It wouldn't hurt as much as the headache. This is not the first episode of this type of headache. They seem to be cyclical in nature. He can have several attacks in one day, and they last from 15 minutes to 3 hours over the course of several days, and then go for weeks without a headache. He has tried to manage them with over the counter meds, but admitted the medications did not help. An MRI of the brain was ordered to rule out an ischemic event. The MRI was negative. While waiting for the MRI results, the patient was noted to be rocking back and forth on the bed, as if attempting to soothe himself. Pain meds were ordered and seemed to provide some relief, though it is not known if the headache just resolved itself or if the medication was truly effective. Based on symptomology and the patient's description of the headaches, he was diagnosed with episodic cluster headaches.
First-listed diagnosis: ________
Secondary diagnoses: ________
Fill in the blank with correct word.
Question 2
Martin is 69 years old, and has a long-standing history of COPD brought on by years of smoking. He finally stopped smoking about four years ago when he retired. In addition to the COPD, Martin has hypertensive heart disease and chronic atrial fibrillation. He was admitted to the hospital directly from his physician's office. At the time of admission, he had dyspnea, tachycardia, and yellowish sputum. He was treated with medications and respiratory therapy. His hypertension was well controlled throughout his stay and the chronic a-fib was managed with his usual medications. After several days of treatment, he was discharged home with a diagnosis of acute exacerbation of COPD.
First-listed diagnosis: ________
Secondary diagnoses: ________
Fill in the blank with correct word.

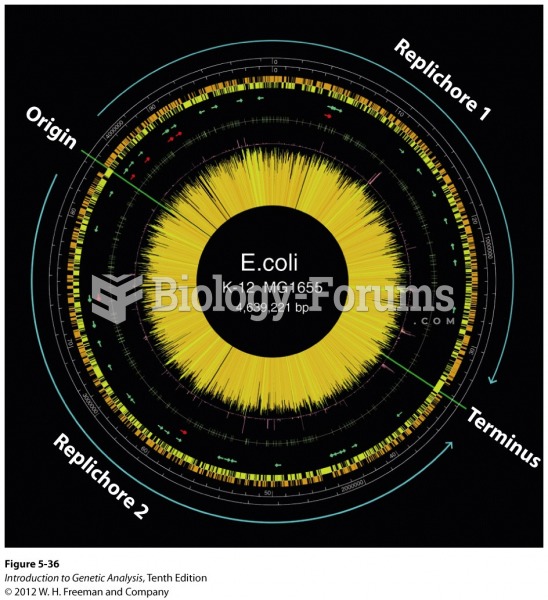 Physical map of the E. coli genome
Physical map of the E. coli genome
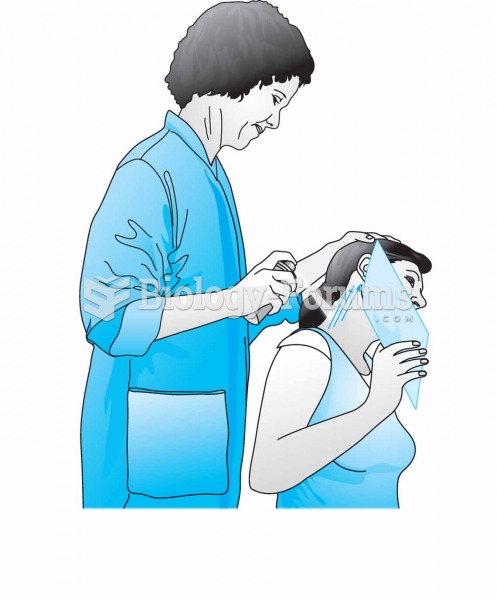 Vapocoolant spray application while passively stretching the paracervical muscles. Take care to prot
Vapocoolant spray application while passively stretching the paracervical muscles. Take care to prot
 Helping maintain accurate patient records is a critical part of the medical assistant's work.
Helping maintain accurate patient records is a critical part of the medical assistant's work.
 A physical therapist helping the patient on parallel bars.
A physical therapist helping the patient on parallel bars.
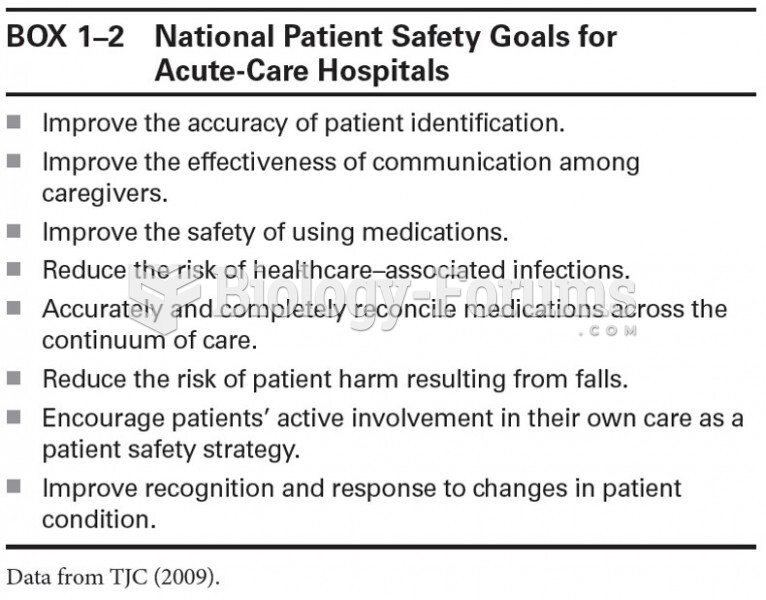 National Patient Safety Goals for Acute-Care Hospitals
National Patient Safety Goals for Acute-Care Hospitals