Answer to Question 1
B
Feedback:
The timing of administration of narcotics in labor is especially important. If given close to birth, because the fetal liver takes 2 to 3 hours to activate a drug, the effect will not be registered in the fetus for 2 to 3 hours after maternal administration. For this reason, narcotics are preferably given when the mother is more than 3 hours away from birth. This allows the peak action of the drug in the fetus to have passed by the time of birth. The nurse does not need to get permission from the physician. Pain medication can be provided when needed and not on a set schedule of every 4 hours. The patient is nearing delivery so 3 hours from the last dose will not influence the decision to provide more medication.
Answer to Question 2
B
Feedback:
The role of the nurse should be to support the woman in her choice of pushing method and to encourage confidence in her maternal instinct of when and how to push. In the absence of any complications, nurses should not be controlling this stage of labor, but empowering women to achieve a satisfying experience. Common practice in many labor units is still to coach women to use closed glottis pushing with every contraction, starting at 10 cm of dilation, a practice that is not supported by research. Research suggests that directed pushing during the second stage may be accompanied by a significant decline in fetal pH and may cause maternal muscle and nerve damage if done too early. Effective pushing can be achieved by assisting the woman to assume a more upright or squatting position. Supporting spontaneous pushing and encouraging women to choose their own method of pushing should be accepted as best clinical practice.

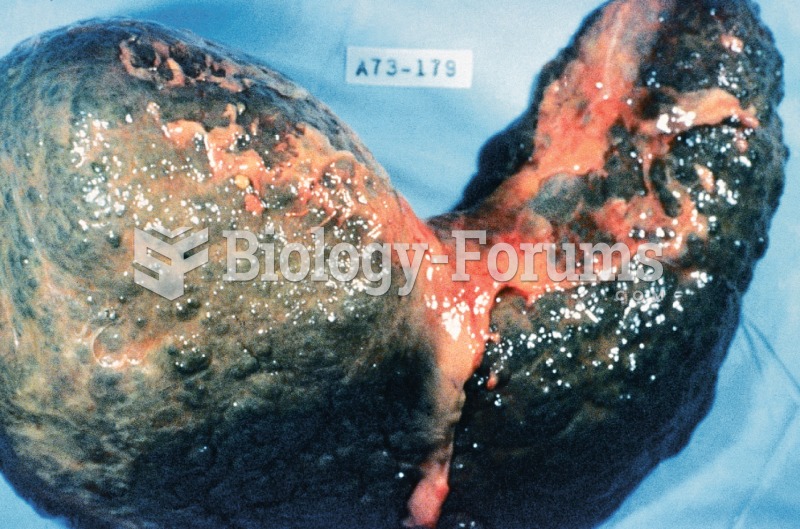 Cirrhosis. Cirrhosis is characterized by a chronic deterioration of the liver, replacing healthy cel
Cirrhosis. Cirrhosis is characterized by a chronic deterioration of the liver, replacing healthy cel
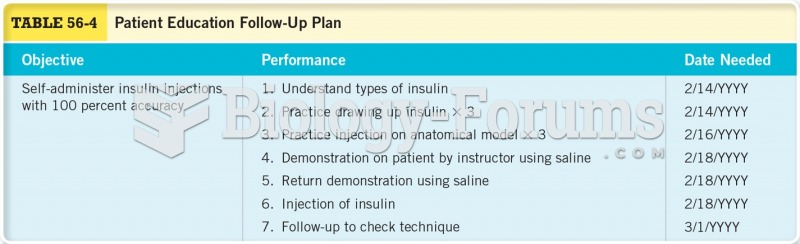 Patient Education Follow-up Plan
Patient Education Follow-up Plan
 ROM exercises on a patient’s wrist: flexion.
ROM exercises on a patient’s wrist: flexion.
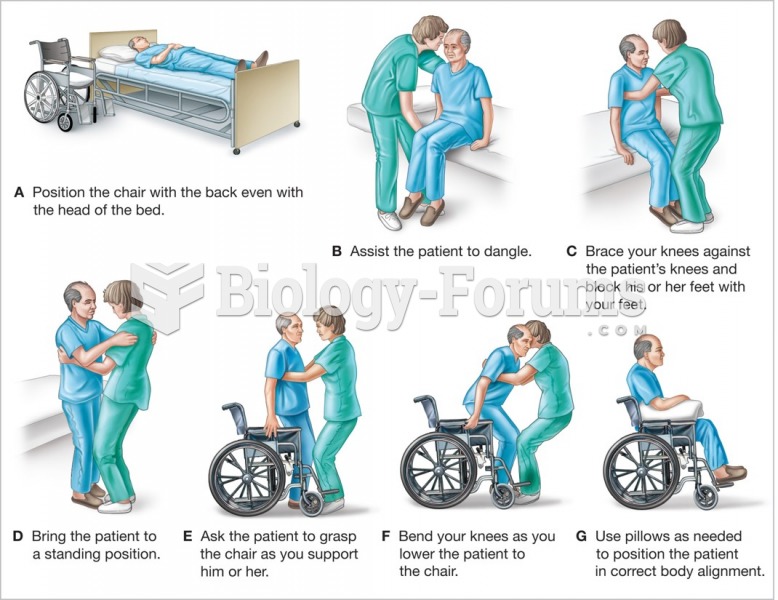 Assisting the patient to transfer from the bed or examining table to a wheelchair.
Assisting the patient to transfer from the bed or examining table to a wheelchair.
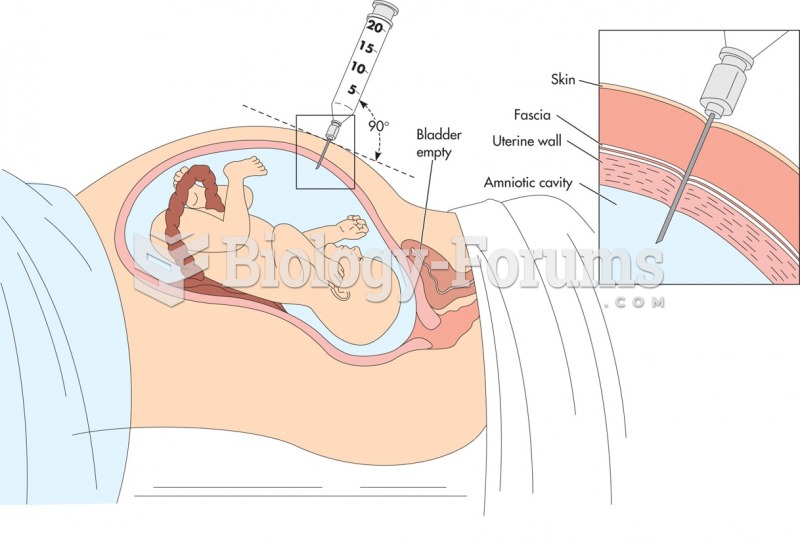 Amniocentesis. The patient is examined with ultrasound to determine the placental site and to locate ...
Amniocentesis. The patient is examined with ultrasound to determine the placental site and to locate ...
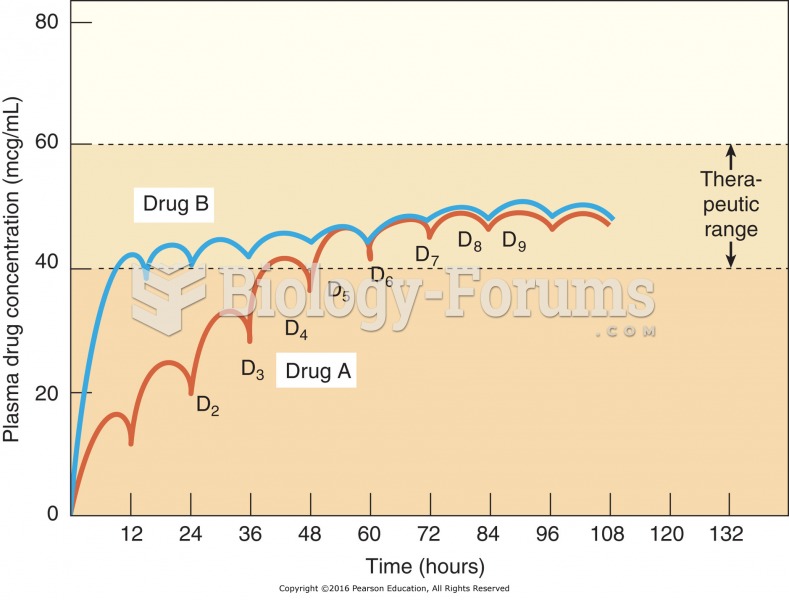 Multiple-dose drug administration. Drug A and drug B are administered every 12 hours. Drug B reaches ...
Multiple-dose drug administration. Drug A and drug B are administered every 12 hours. Drug B reaches ...