Answer to Question 1
ANS: C
Many children obtain significantly less sleep in the hospital than at home; the primary causes are a delay in sleep onset and early termination of sleep because of hospital routines. One technique that can minimize the disruption in the child's routine is establishing a daily schedule. This approach is most suitable for noncritically ill school-age and adolescent children who have mastered the concept of time. It involves scheduling the child's day to include all those activities that are important to the child and nurse, such as treatment procedures, schoolwork, exercise, television, playroom, and hobbies. The school-age child with osteomyelitis would benefit from a schedule similar to the one followed at home. Requesting a prescription for a sleeping pill would be inappropriate, and allowing the child to stay up late and sleep late would not be keeping the child in a routine followed at home. Passive activities in the morning and interactive activities at bedtime should be reversed; it would be better to keep the child active in the morning hours and plan quiet activities at bedtime.
Answer to Question 2
ANS: C
When a child is admitted, nurses follow several fairly universal admission procedures. The minimum considerations for room assignment are age, sex, and nature of the illness. Age-grouping is especially important for adolescents. The 14-year-old boy being admitted to the unit after appendectomy surgery should be placed with a noninfectious child of the same sex and age. The 15-year-old child with sickle cell is the best choice. The 4-year-old boy who is post-appendectomy is too young, and the child with pneumonia is too young and possibly has an infectious process. The 12-year-old boy with cellulitis is the right age, but he has an infection (cellulitis).

 Measles. A photograph of a child stricken with measles, showing the tell-tale sign of the skin rash.
Measles. A photograph of a child stricken with measles, showing the tell-tale sign of the skin rash.
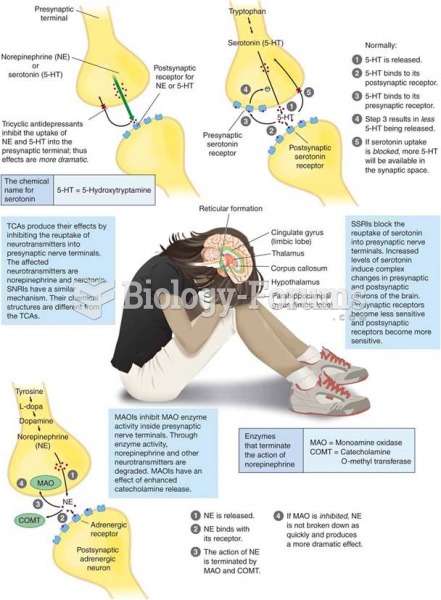 Antidepressant Therapy Is Directed Toward the Amelioration of Depressive Symptoms
Antidepressant Therapy Is Directed Toward the Amelioration of Depressive Symptoms
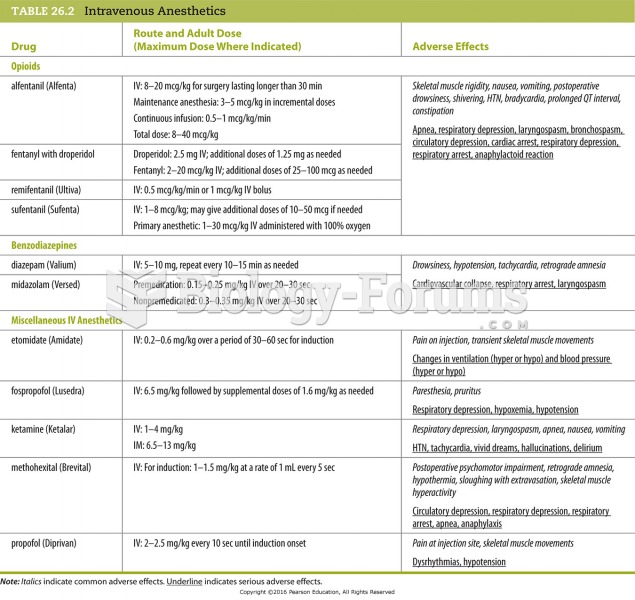 Intravenous Anesthetics
Intravenous Anesthetics
 Cost of Going to School
Cost of Going to School
 Therapy Animals
Therapy Animals
 Genetic therapy for mice with Duchenne muscular dystrophy
Genetic therapy for mice with Duchenne muscular dystrophy