Answer to Question 1
A
Answer to Question 2
Important Points:
During the diuretic phase of acute kidney injury, the kidneys are unable to concentrate urine and urine output increases to as much as 5 L/day.
The patient may develop dehydration and hypovolemia, with potential shock and recurrent kidney injury.
The kidney continues to be unable to perform other functions, such as remove metabolic wastes, control acid-base balance, and maintain normal electrolyte levels.
The patient may develop hyponatremia and hypokalemia during this phase.
Nursing and collaborative interventions include:
Careful assessment for manifestations of dehydration and hypovolemia: vital sign changes, such as hypotension and tachycardia, poor pulse quality, flat neck veins, dry oral mucosa, poor skin turgor, and changes in orientation and alertness.
Assessment for electrolyte disturbances, such as hyponatremia or hypokalemia caused by diuresis.
Infusion of fluids (based on the patient's I & O and fluid balance) and monitoring for signs of fluid excess, such as hypotension or hypertension, tachycardia, increased respiratory rate and dyspnea, crackles in the lungs, pericardial and pleural friction rubs, peripheral edema, and increases in daily weights.

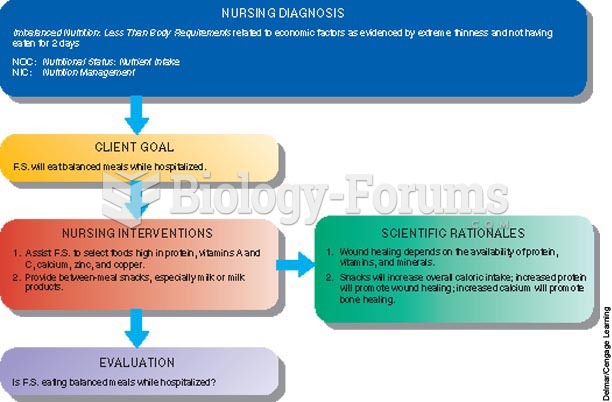 Concept Care Map
Concept Care Map
 Assessment of stereognosis.
Assessment of stereognosis.
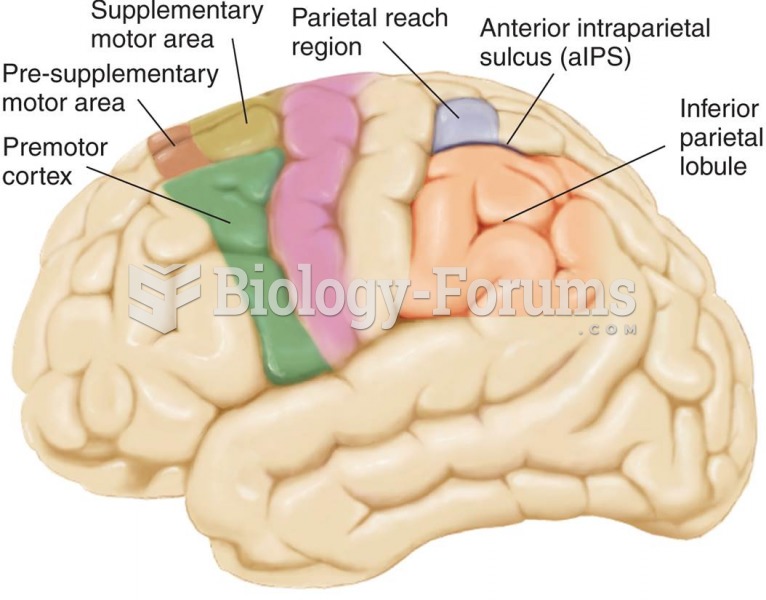 Important Motor Regions of the Human Brain
Important Motor Regions of the Human Brain
 Among the health benefits of marriage is a longer life.
Among the health benefits of marriage is a longer life.
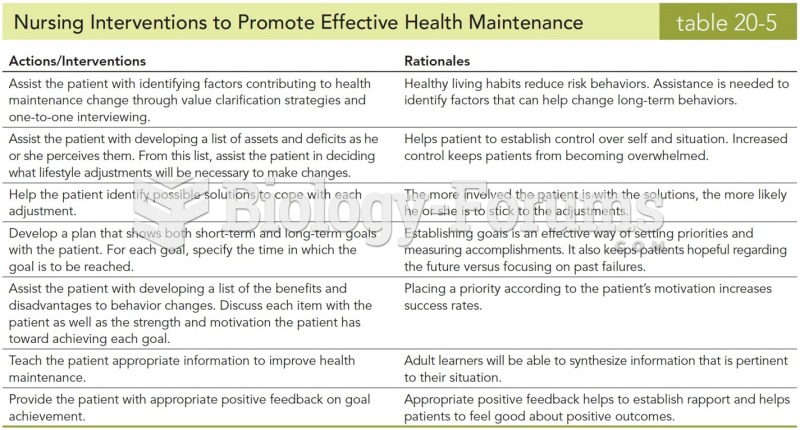 Nursing Interventions to Promote Effective Health Maintenance
Nursing Interventions to Promote Effective Health Maintenance