Answer to Question 1
ANS: D
Category Factor Mechanism Clinical Presenta-tion
Cardiac status Acute left-ventricular fail-ure Increased preload because of in-creased venous re-turn and decreased pulmonary capillary compression as in-trathoracic pressure is reduced. Weaning fails, often after patient does well initially for 30-60 minutes; may develop acute res-piratory and/or metabolic acidosis, hypoxemia, hypo-tension, chest pain, and cardiac dysrhythmias.
Acid-base status Acute alkalosis in patient with under-lying carbon diox-ide (CO2) retention Loss of preexisting metabolic compen-sation for hyper-capnia; inability to sustain required and WOB. Patient with COPD or other cause of chronic respiratory acidosis before acute insult fails weaning after sev-eral days of ventila-tion to a PaCO2 lower than the pa-tient's pH-compensated level.
Respiratory alkalo-sis Depression of ven-tilatory drive by hypocapnia and al-kalemia. PaCO2 rises and pH falls during wean-ing attempt; patient is said to fail wean-ing if some arbitrary change in these values (e.g., 10 mm Hg increase in Pa-CO2) is used as a criterion for failure.
Metabolic acidosis Increase in ventila-tory demand to compensate for res-piratory alkalosis. Patient may be una-ble to sustain re-quired increase in and WOB to main-tain a lower PaCO2 to compensate for a lower HCO3.
Metabolic status Hypophosphatemia and hypomagnese-mia Ventilatory muscle weakness. Patient weaning fails because of rapid shallow breathing, respira-tory distress, and acute respiratory acidosis; maximal inspiratory pressure is decreased.
Hypothyroidism Decreased ventila-tory drive with pos-sible ventilatory muscle weakness. Rare cause of weaning failure that occurs because of acute respiratory acidosis with or without respiratory distress.
Drugs Narcotics, seda-tives, tranquilizers, and hypnotics Depression of ven-tilatory drive. Patient fails wean-ing because of acute respiratory acidosis in the absence of tachypnea and res-piratory distress.
Neuromuscular blocking agents Ventilatory muscle weakness; delayed clearance in patient with renal insuffi-ciency. Patient weaning fails because of rapid shallow breathing, respira-tory distress, and acute respiratory acidosis; maximal inspiratory pressure is reduced.
Ventilatory muscle weakness caused by acute myopathy, especially in pa-tients who have re-ceived high-dose systemic cortico-steroids. Same as above; may have elevated mus-cle enzymes; can last for weeks or months.
Aminoglycosides Neuromuscular blockade. Very rare cause of weaning failure that occurs because of rapid shallow breathing, respira-tory distress, and acute respiratory acidosis; maximal inspiratory force is reduced.
Nutrition Overfeeding Increased CO2 production, espe-cially with exces-sive carbohydrate calories. Patient fails wean-ing because of ex-cessive ventilatory demand (high re-quirement to keep PaCO2 normal); un-usual cause of weaning failure un-less very large ca-loric loads are ad-ministered.
Malnutrition Effects of acute illness; preexisting nutritional deficien-cies. May contribute to ventilatory muscle weakness, de-creased ventilatory drive, impaired immunologic func-tion, fluid retention, depression; distin-guishing this from other factors is dif-ficult.
Psychological status Agitation; psy-chological ventilator dependence Anxiety, fear, de-lirium, ICU psycho-sis, or influence of preexisting person-ality factors. Patient becomes agitated and pan-icky during attempt to reduce or discon-tinue ventilatory support; can be said to cause weaning failure when other factors are absent.
Lack of motivation Depression, effects of drugs, organic brain dysfunction, or influence of preexisting person-ality factors. Patient refuses to participate in care (e.g., mobilization, bronchial hygiene, physiological meas-urements); flat af-fect and immobility in bed; considered when other factors are absent.
Answer to Question 2
ANS: C
The cuff leak test is a means of testing for post-extubation airway patency. Note that to qualify for this test, the patient must no longer need ventilatory support. To perform this test, the patient is disconnected from the ventilator, the cuff is deflated, and the ET or tracheostomy tube is ob-structed. A leak around the cuff (peritubular leak) during spontaneous breathing suggests that the airway caliber is adequate and successful extubation is likely. A leak of less than 110 mL (aver-age of three values on six consecutive breaths) indicates a high risk of post-extubation stridor. Treatment with steroids or racemic epinephrine (or both) before extubation may be indicated.

 Treating the pregnant patient
Treating the pregnant patient
 All messages must be documented and placed in the patient's chart.
All messages must be documented and placed in the patient's chart.
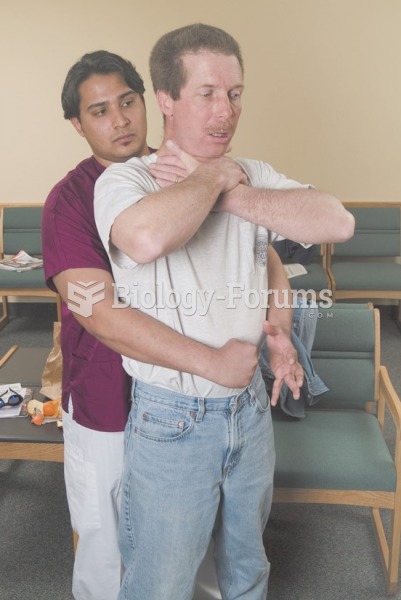 Abdominal thrusts are delivered with a firm thrust into the patient’s abdomen with an upward ...
Abdominal thrusts are delivered with a firm thrust into the patient’s abdomen with an upward ...
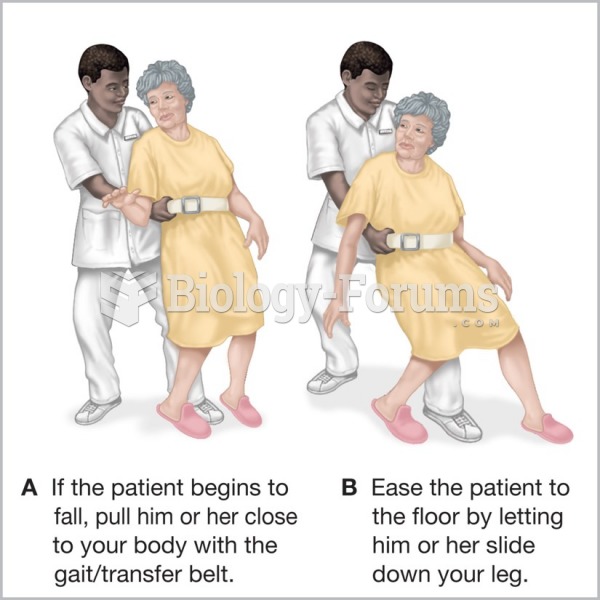 Assisting a falling patient.
Assisting a falling patient.
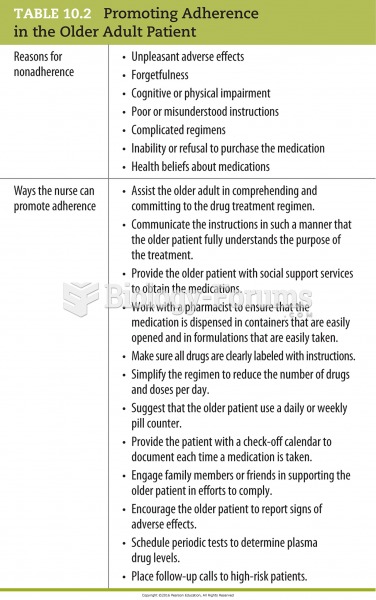 Promoting Adherence in the Older Adult Patient
Promoting Adherence in the Older Adult Patient
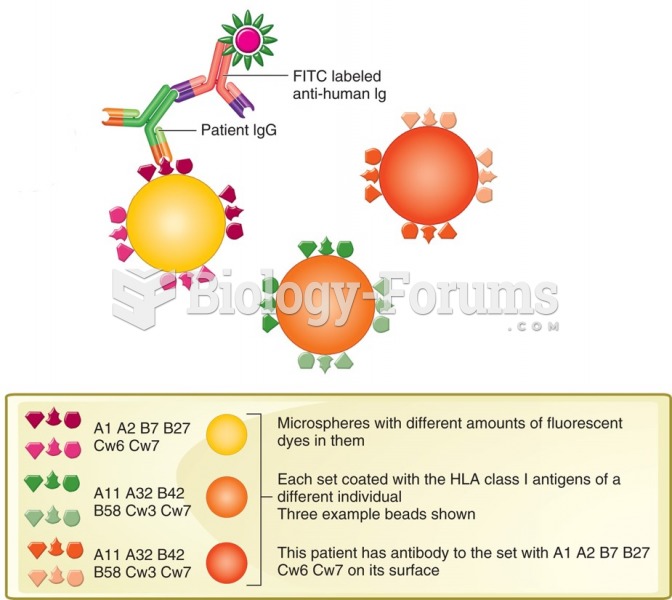 Colorimetric multiplex assay to determine anti-HLA antibodies in a patient's serum.
Colorimetric multiplex assay to determine anti-HLA antibodies in a patient's serum.