A patient with a past medical history of COPD was placed on a ventilator after upper abdominal surgery for a serious wound infection.
Although the patient was medically stable, a tracheostomy was performed 2 weeks later because the patient was unable to be weaned from the ventilator. The patient is on VC-CMV, rate = 12, VT = 700 mL, FIO2 = 40, PEEP = 5 cm H2O, with an HME. The respiratory therapist notes that the patient is assisting at a rate of 18 and has bilaterally decreased breath sounds in the bases. The respiratory therapist suctions a moderate amount of very thick, tenacious yellow sputum from the tracheostomy tube. What action should the respiratory therapist take?
a. The HME should be replaced with an active heated humidifier system.
b. No action is necessary, because there seems to be no patient problem.
c. The patient should be suctioned on a regular schedule instead of when needed.
d. PEEP and the FIO2 should be increased, and diuretic and positive inotropic agents should be administered.
Question 2
An intubated patient is receiving mechanical ventilation with the following settings: VC-CMV, rate = 18, VT = 850 mL (10 mL/kg), PEEP = 5 cm H2O, flow rate = 40 L/min. The patient is se-dated and is not assisting the ventilator.
During a patient-ventilator system check, the respiratory therapist observes the following venti-lator graphic:
The respiratory therapist should do which of the following?
a. Decrease the flow rate.
b. Increase the PEEP.
c. Decrease the rate.
d. Increase the VT.

 upper body
upper body
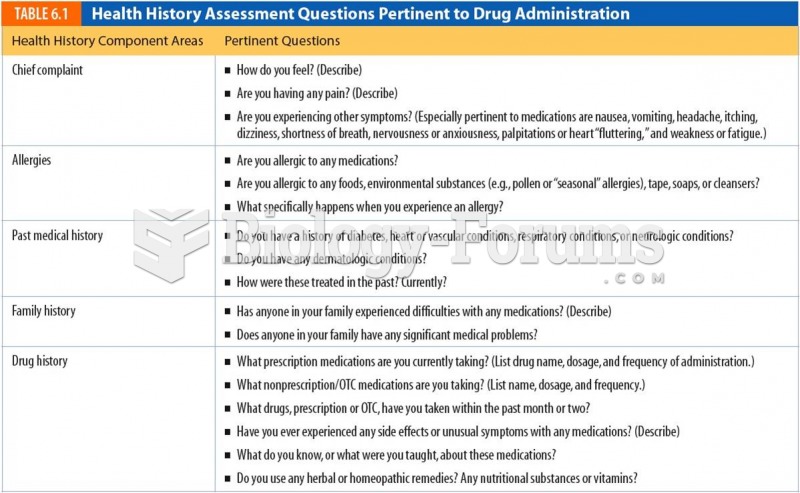 Health History Assessment Questions Pertinent to Drug Administration
Health History Assessment Questions Pertinent to Drug Administration
 History Vector Icon
History Vector Icon
 Prepare upper back for hot application. Undrape upper back. Check tissues visually and through ...
Prepare upper back for hot application. Undrape upper back. Check tissues visually and through ...