Answer to Question 1
ANS: D
Laboratory CO-oximeters measure four types of hemoglobin: oxyhemoglobin (O2Hb), deoxy-genated hemoglobin (HHb), carboxyhemoglobin (COHb), and methemoglobin (MetHb). This is beneficial for patients who are suffering from smoke inhalation. The CO-oximeter provides the actual O2Hb and the COHb. Carbon monoxide produces an erroneously high oxygen saturation measured by pulse oximeter (SpO2). Therefore, if smoke inhalation is suspected, a CO-oximeter should be used to evaluate the oxygen saturation. Capnography is the measurement of carbon dioxide concentrations in exhaled gases and is used to assess proper airway placement. Calorime-try allows the clinician to estimate energy expenditure from measurements of oxygen consump-tion (O2) and carbon dioxide production (CO2). This measurement may be useful when weaning a patient from mechanical ventilation.
Answer to Question 2
ANS: C
The oxygen status of a patient being considered for extubation needs to be assessed by an arterial blood gas, not by pulse oximetry, because not only does the patient's oxygen status need assess-ment, but the acid-base balance does as well. Pulse oximetry is not used as a basis for prescribing oxygen therapy in neonates. Neonatologists prefer to base oxygen therapy decisions on arterial partial pressure of oxygen (PaO2) rather than oxygen saturation. Pulse oximetry is useful for mon-itoring the oxygen status of patients undergoing chest physical therapy because it gives immedi-ate results and is used for continuous monitoring. Pulse oximetry may not be as useful in pre-scribing oxygen therapy for home care patients.

 Taking a Patient’s Oral Temperature with an Electronic Thermometer
Taking a Patient’s Oral Temperature with an Electronic Thermometer
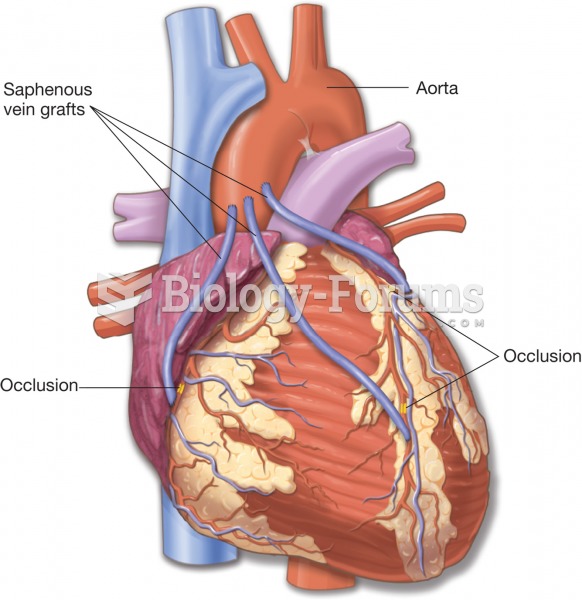 Coronary artery bypass graft (CABG). The grafts are often obtained from the patient’s saphenous vein
Coronary artery bypass graft (CABG). The grafts are often obtained from the patient’s saphenous vein
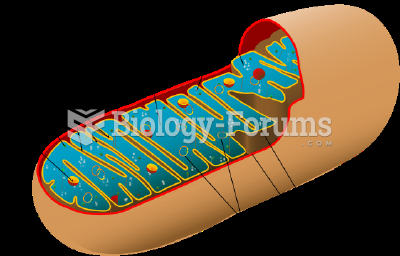 Mitochondria known as power house of the cell
Mitochondria known as power house of the cell
 Preparing the Patient’s Skin for Surgical Procedures
Preparing the Patient’s Skin for Surgical Procedures
 Pneumonia patient’s chest x-ray. Note the irregular areas of density.
Pneumonia patient’s chest x-ray. Note the irregular areas of density.
 Still Life, House of The Stags (Cervi)
Still Life, House of The Stags (Cervi)