Answer to Question 1
ANS: A
Both the assessment and blood gas results reveal that the patient is spontaneously breathing. However, it appears that the patient is suffering from air hunger. The blood gases reveal that the patient has refractory hypoxemia. With this information, the most appropriate recommenda-tion would be to place the patient on continuous positive airway pressure (CPAP) with supple-mental oxygen to improve the refractory hypoxemia by opening up atelectatic areas and main-taining them open. Since the patient is breathing spontaneously, mechanical ventilator breaths are not necessary.
Answer to Question 2
ANS: C
Switching to pressure-controlled ventilation will reduce the continued risk of alveolar overdisten-tion, which has already caused a pneumothorax, by limiting the amount of positive pressure ap-plied to the lung. Using the intermittent mandatory ventilation (IMV) mode will decrease the ability of the patient to cause ventilator-induced hyperventilation by triggering mandatory breaths. IMV, with a low ventilator rate setting, can very well reduce this patient's respiratory alkalosis. Using pressure support with the pressure- controlled intermittent mandatory ventilation (PC-IMV) mode will decrease the WOB for the patient during spontaneous breaths.

 Documenting the health history is a crucial step in providing patient care
Documenting the health history is a crucial step in providing patient care
 A Patient Being Prepared for Electroconvulsive Therapy.
A Patient Being Prepared for Electroconvulsive Therapy.
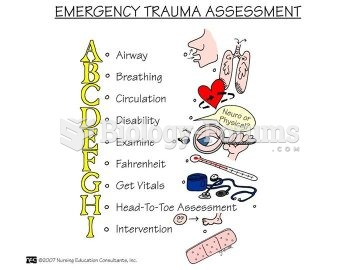 EMERGENCY TRAUMA ASSESSMENT MADE EASY
EMERGENCY TRAUMA ASSESSMENT MADE EASY
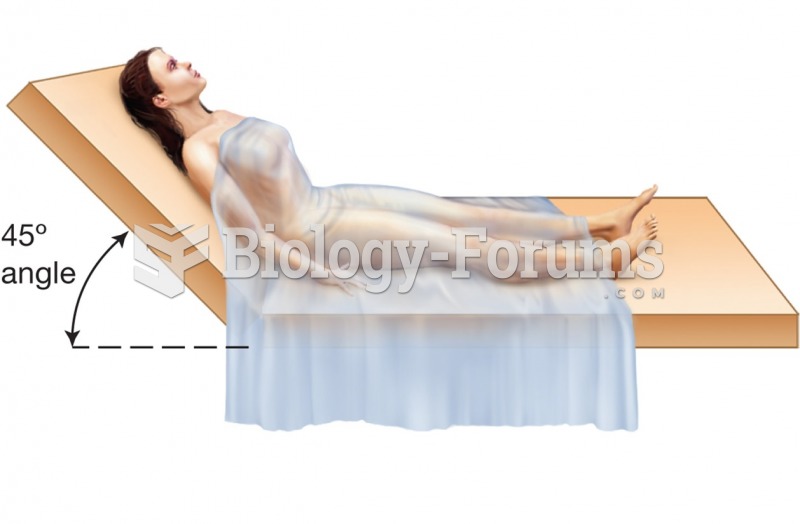 Positioning the Patient in the Fowler’s Position
Positioning the Patient in the Fowler’s Position
 Preparing the Patient’s Skin for Surgical Procedures
Preparing the Patient’s Skin for Surgical Procedures