This topic contains a solution. Click here to go to the answer
|
|
|

 Nurses may collaborate with social workers, physicians, and other members of the health care team to
Nurses may collaborate with social workers, physicians, and other members of the health care team to
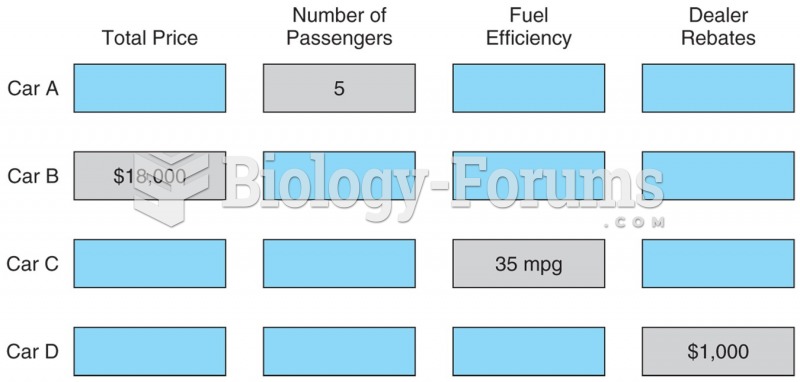 Example of a choice board used in studies of decision making. This one includes four factors for ...
Example of a choice board used in studies of decision making. This one includes four factors for ...
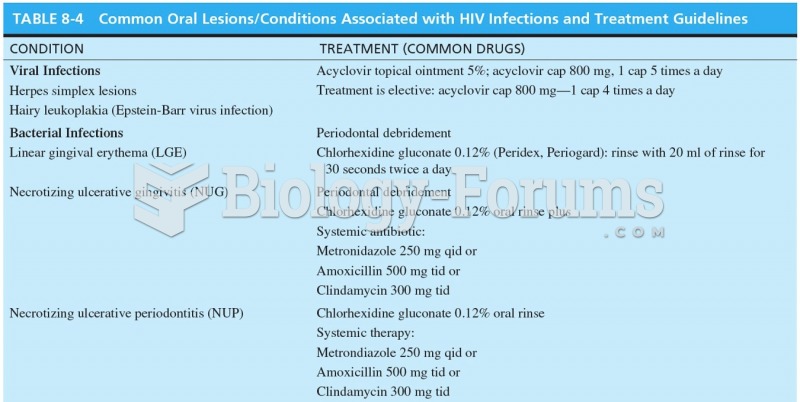 Common Oral Lesions/Conditions Associated with HIV Infections and Treatment Guidelines
Common Oral Lesions/Conditions Associated with HIV Infections and Treatment Guidelines
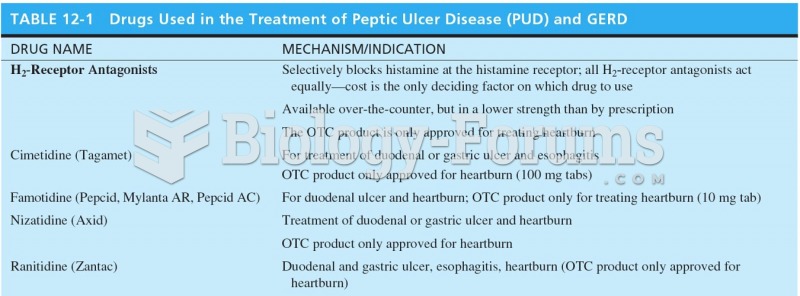 Drugs Used in the Treatment of Peptic Ulcer Disease (PUD) and GERD
Drugs Used in the Treatment of Peptic Ulcer Disease (PUD) and GERD
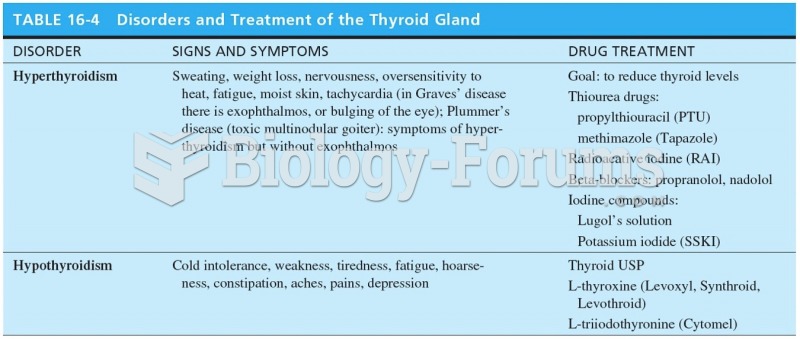 Disorders and Treatment of the Thyroid Gland
Disorders and Treatment of the Thyroid Gland
 Apply the substance to the client’s upper chest.
Apply the substance to the client’s upper chest.