Answer to Question 1
A
Feedback:
If wound disruption is suspected, the nurse should position the client to put the least strain on the operated area. The nurse should inform the physician immediately rather than informing the head nurse first. If evisceration occurs, the nurse places sterile dressings moistened with normal saline over the protruding organs and tissues. The nurse must be alert for signs and symptoms of impaired blood flow such as swelling, localized pallor or a mottled appearance, and coolness of the tissue in the area around the wound. Palpation of the wound would be an inappropriate action in this case.
Answer to Question 2
B
Feedback:
The nursing kardex provides a succinct and accessible record of many aspects of a client's current orders. The care plan would address the issue of mobility but may not specify the current orders for the client's activity at this point in recovery. Checklists and flow sheets are not places where current orders are recorded and updated.

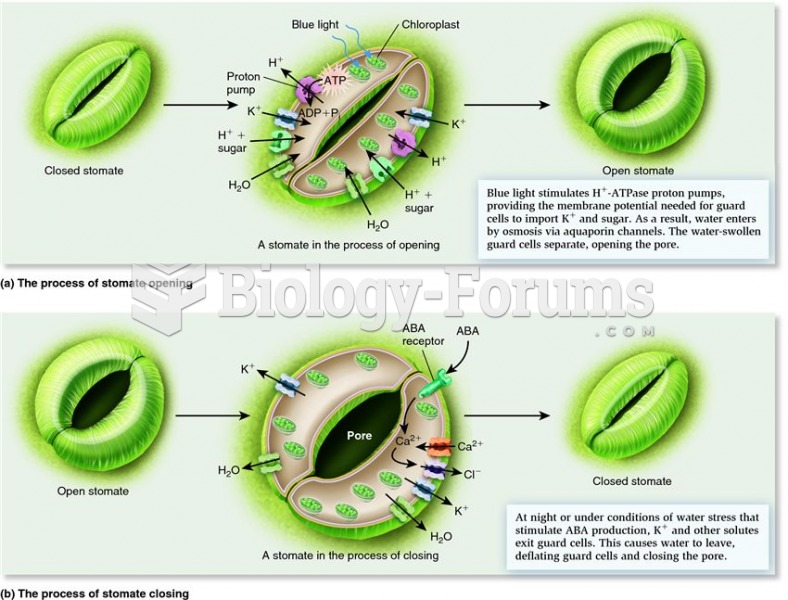 How stomatal pores open and close.
How stomatal pores open and close.
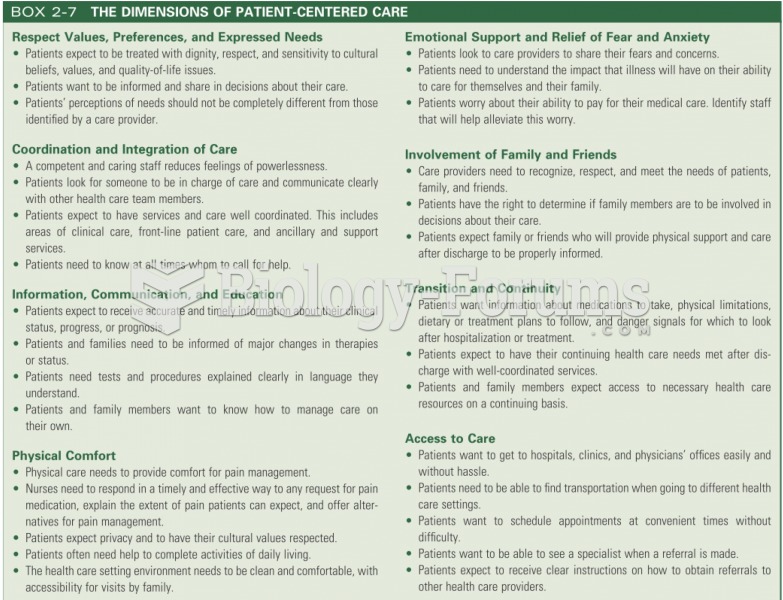 THE DIMENSIONS OF PATIENT-CENTERED CARE
THE DIMENSIONS OF PATIENT-CENTERED CARE
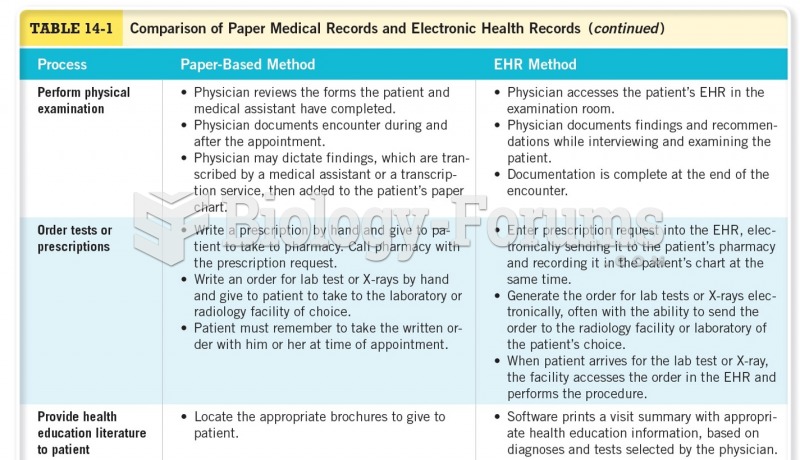 Comparison of Paper Medical Records and Electronic Health Records
Comparison of Paper Medical Records and Electronic Health Records
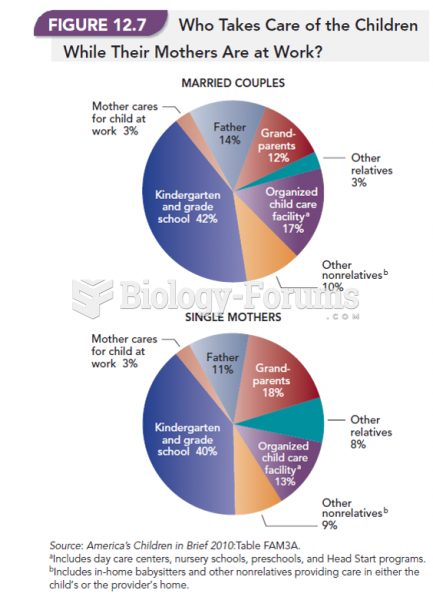 Who Takes Care of the Children While the Mothers Are at Work?
Who Takes Care of the Children While the Mothers Are at Work?
 Nurse administering enteral nutrition through a feeding tube.
Nurse administering enteral nutrition through a feeding tube.
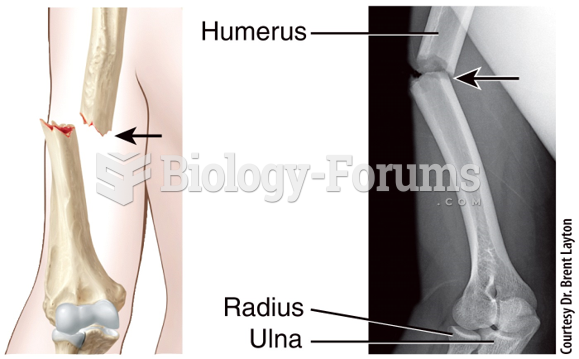 Fracture and Repair of Bone Open (Compound)
Fracture and Repair of Bone Open (Compound)