Answer to Question 1
A
Feedback
A If the patient has unilateral weakness, the nurse should place food in the stronger side of the mouth.
B The patient should be positioned in an upright, seated position to prevent aspiration.
C Patients with unilateral weakness often have difficulty using a straw.
D Thickened liquids are often tolerated better and will help prevent aspiration, as patients with impaired swallowing often choke more with thin liquids.
Answer to Question 2
C
Feedback
A Reassessment may not require redoing the entire care plan.
B The nurse should not focus only on the nursing diagnoses and goals that have changed; nursing interventions may also need revising to meet new goals. Adding more nursing interventions may or may not be necessary. The nurse adjusts interventions on the basis of the client's response and the nurse's previous experience with similar clients.
C A complete reassessment of all client factors relating to the nursing diagnosis and etiology is necessary when modifying a plan. After reassessment, the nurse will determine what components of the care plan are accurate for the situation.
D Standards of care are used to determine whether the right interventions have been chosen or whether additional ones are required.

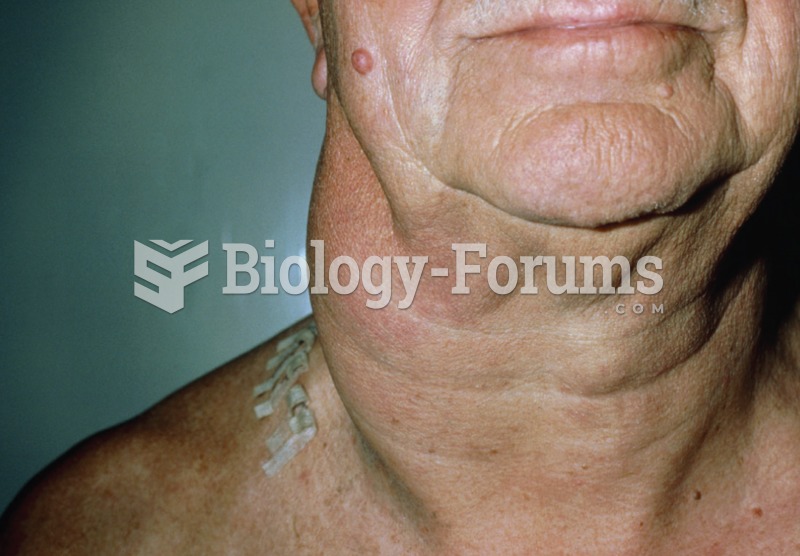 Photo of the neck of a patient with non-Hodgkin’s lymphoma showing the swelling associated with enla
Photo of the neck of a patient with non-Hodgkin’s lymphoma showing the swelling associated with enla
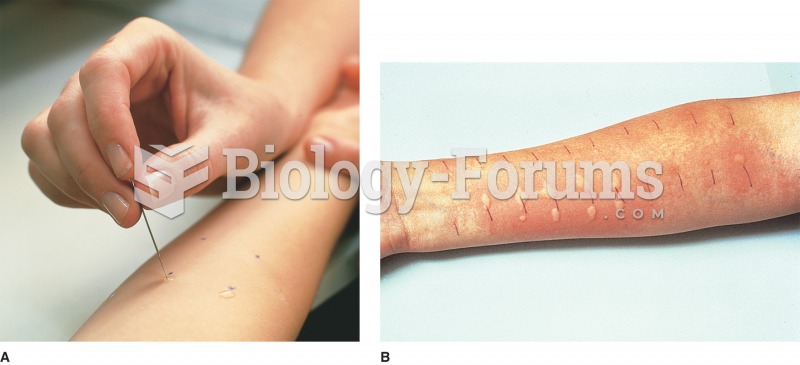 (A) Scratch test; patient is exposed to allergens through a light scratch on the skin; (B) Positive
(A) Scratch test; patient is exposed to allergens through a light scratch on the skin; (B) Positive
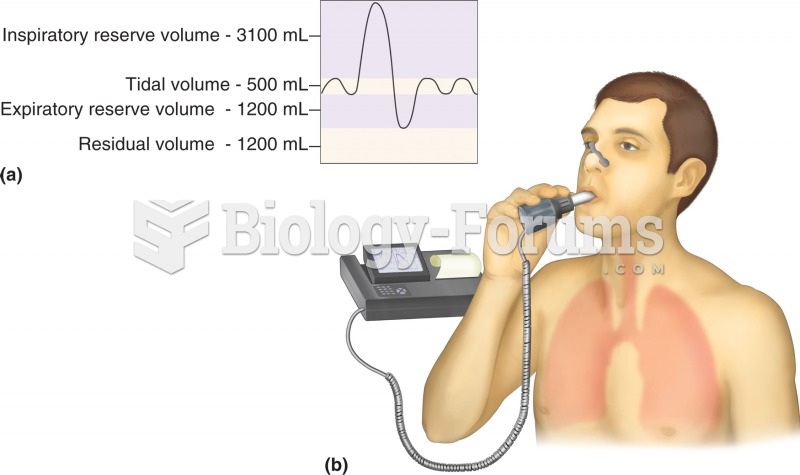 Pulmonary function test: spirometry. (a) Normal respiratory volumes, as measured during spirometry.
Pulmonary function test: spirometry. (a) Normal respiratory volumes, as measured during spirometry.
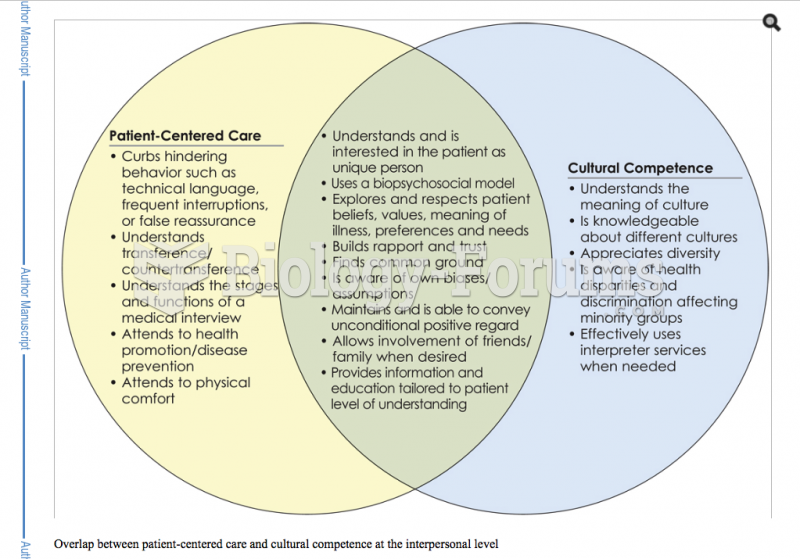
 Building competency in patient centered care
Building competency in patient centered care
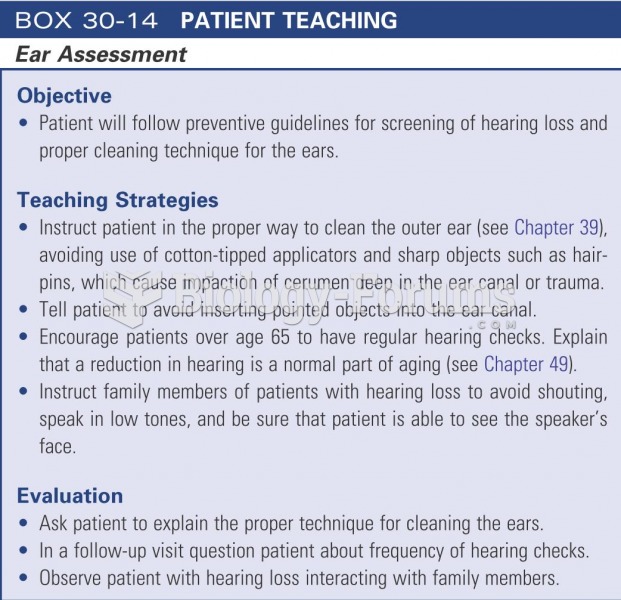 Patient teaching: ear assessment
Patient teaching: ear assessment
 Health care - patient-centered
Health care - patient-centered