Answer to Question 1
ANS: A
The MMSE is a formal diagnostic tool that is used to assess a patient's level of cognitive functioning. The Mini-Mental State Examination (MMSE) is a tool you can use to measure disorientation, change in problem-solving abilities, and altered conceptualization and abstract thinking. Asking the patient orientation questions evaluates only the patient's orientation to self and surroundings, not abstract reasoning or critical thinking ability. Family members are not the most reliable source of information about the patient, although information received from the family should be considered. The HHIE-S is a 5-minute, 10-item questionnaire that assesses how the individual perceives the social and emotional effects of hearing loss. The higher the HHIE-S score, the greater the handicapping effect of a hearing impairment.
Answer to Question 2
ANS: C
A visual disturbance poses great risk for injury due to falling from impaired depth perception and inability to see obstacles. Body image disturbance, social isolation, and fear are all valid nursing diagnoses that apply to a patient with vision deficit; however, they do not address the greatest risk for injury.

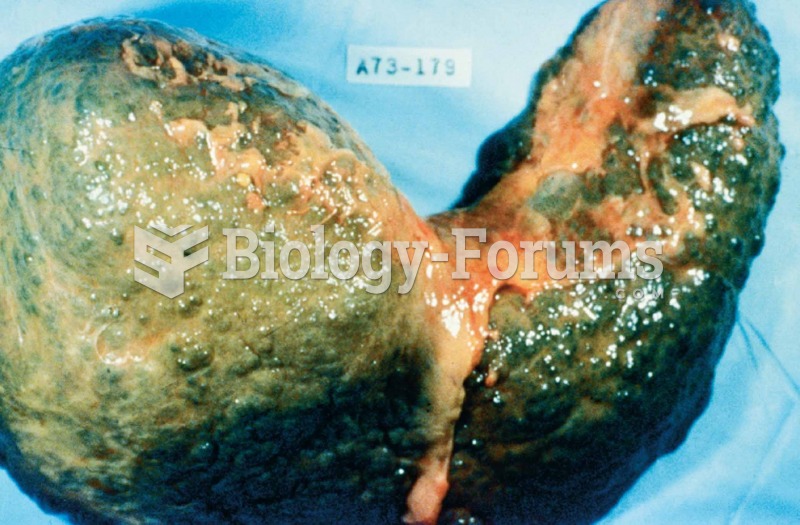 The liver in this photograph was from a deceased patient with an advanced state of cirrhosis.
The liver in this photograph was from a deceased patient with an advanced state of cirrhosis.
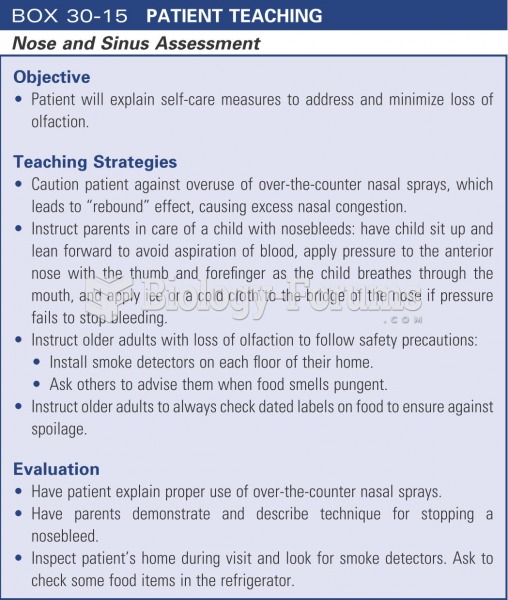 Patient teaching: nose and sinus assessment
Patient teaching: nose and sinus assessment
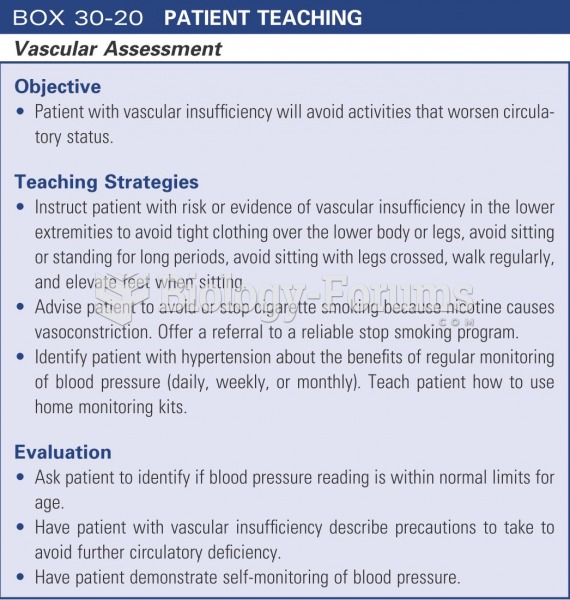 Patient teaching: vascular assessment
Patient teaching: vascular assessment
 It is important to act concerned when a patient is upset.
It is important to act concerned when a patient is upset.
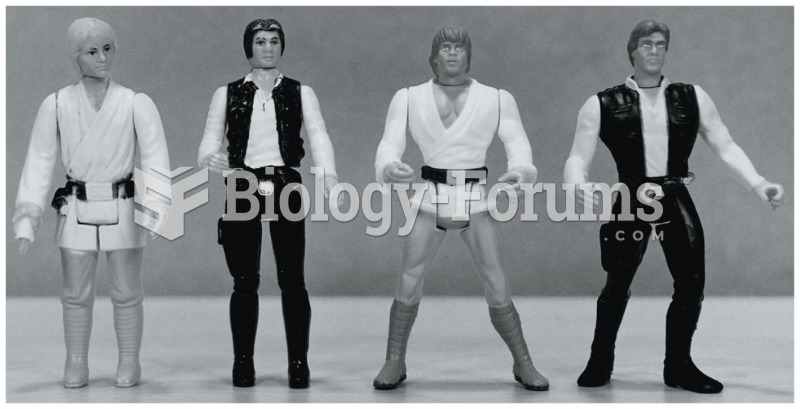 The male physique depicted in popular action figures in the 1970s
The male physique depicted in popular action figures in the 1970s