Answer to Question 1
ANS: B
The term electronic health record/EHR is increasingly used to refer to a longitudinal (lifetime) record of all health care encounters for an individual patient by linking all patient data from previous health encounters. An electronic medical record (EMR) is the legal record that describes a single encounter or visit created in hospitals and outpatient health care settings that is the source of data for the EHR. There are no such terms as electronic charting record or electronic problem record that record the lifetime information of a patient.
Answer to Question 2
ANS: D
Within a computerized documentation system, flow sheets and graphic records allow you to quickly and easily enter assessment data about a patient, such as vital signs, admission and or daily weights, and percentage of meals eaten. In the problem-oriented medical record, the database section contains all available assessment information pertaining to the patient (e.g., history and physical examination, nursing admission history and ongoing assessment, physical therapy assessment, laboratory reports, and radiologic test results). Many computerized documentation systems have the ability to generate a patient care summary document that you review and sometimes print for each patient at the beginning and/or end of each shift; it includes information such as basic demographic data, health care provider's name, primary medical diagnosis, and current orders. Health care team members monitor and record the progress made toward resolving a patient's problems in progress notes.

 A patient with goiter due to iodine deficiency.
A patient with goiter due to iodine deficiency.
 How to find the median of a triangle
How to find the median of a triangle
 How to find the components of a vector found in the first quadrant
How to find the components of a vector found in the first quadrant
 Find Your Blind Spot
Find Your Blind Spot
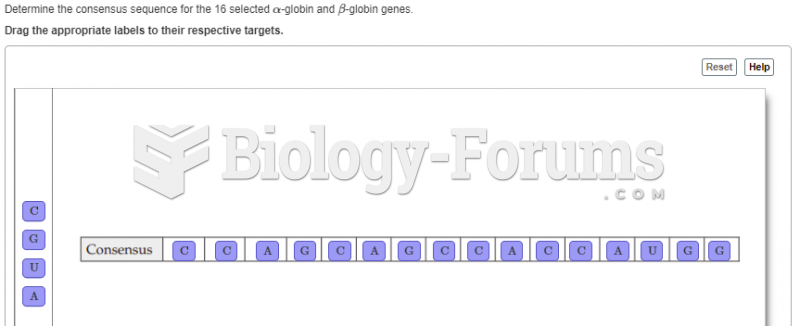 8.The following table contains DNA-sequence information compiled by Marilyn Kozak (1987). The ...
8.The following table contains DNA-sequence information compiled by Marilyn Kozak (1987). The ...
 Locate the following places by reference number on the map:Key Locales of Political, Economic, ...
Locate the following places by reference number on the map:Key Locales of Political, Economic, ...