Answer to Question 1
Correct Answer: 3
Rationale 1: It is never a good idea to leave blanks in any charting area since it implies that the area was ignored.
Rationale 2: It is never a good idea to leave blanks in any charting area. Adding the information in the progress notes is not an appropriate use of that section.
Rationale 3: Many nurses are uncomfortable with the CBE system and believe that if something was not charted, it was not done. A suggestion to address this would be to write N/A on the flow sheets where the items are not applicable to the client, and not leave the spaces blank. This would avoid the possible assumption that the assessment or intervention was not done by the nurse.
Rationale 4: Passing information along in the report is a good way to ensure continuity of care for clients, but this would only be an oral report, not written documentation.
Answer to Question 2
Correct Answer: 4
Rationale 1: Computerized documentation is a way to manage the volume of information required in a client's chart, and different systems may include a variety of setups and programs.
Rationale 2: Focus charting is organized into data, action, and response sections, referred to as DAR.
Rationale 3: SOAP charting is a way to organize data and information in the client's record: S = subjective data; O = objective data; A = assessment; P = plan.
Rationale 4: Charting by exception (CBE) is a documentation system in which only abnormal or significant findings or exceptions to norms are recorded. Flow sheets, standards of nursing care, and bedside access to chart forms are all incorporated into CBE.

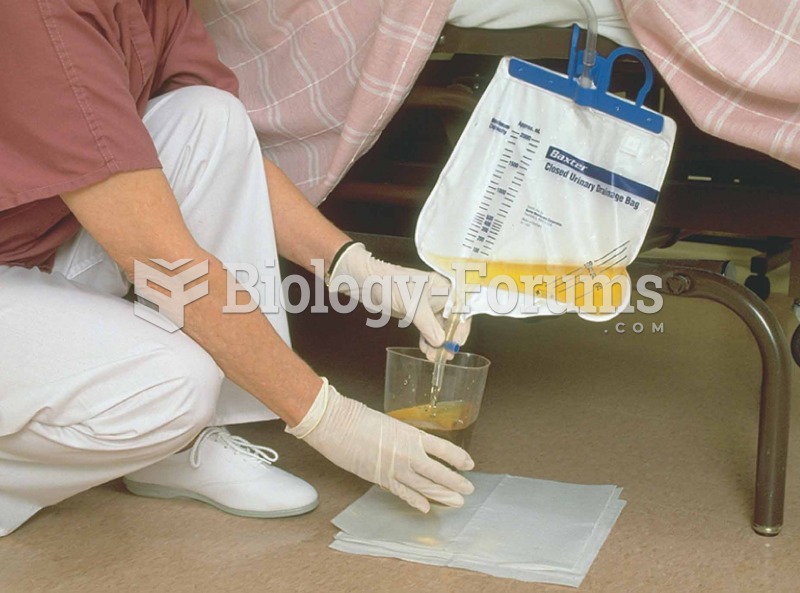 Closed urinary drainage system. Urine being measured after it leaves patient’s body via catheter.
Closed urinary drainage system. Urine being measured after it leaves patient’s body via catheter.
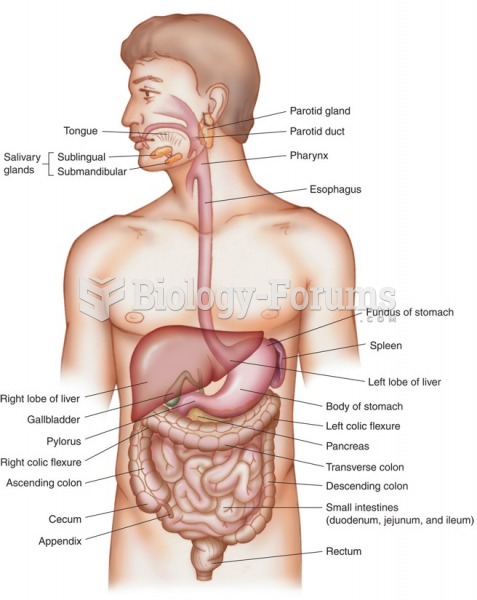 The digestive system.
The digestive system.
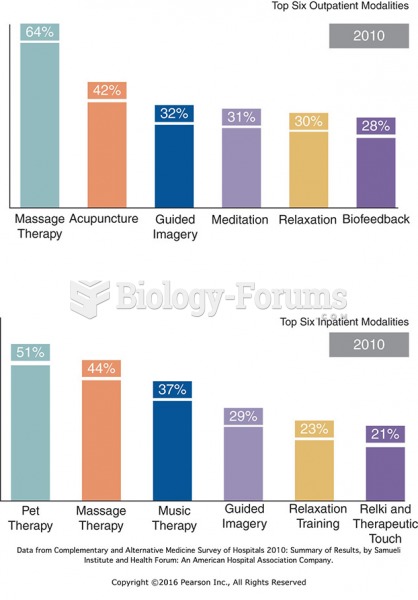 Top Six Hospital Outpatient and Inpatient CAM Therapies.
Top Six Hospital Outpatient and Inpatient CAM Therapies.
 The nurse begins the general survey
The nurse begins the general survey
 The system moves at 1.50 2 m/s while the inclined planes are rough. a) Determine the ...
The system moves at 1.50 2 m/s while the inclined planes are rough. a) Determine the ...