A nursing diagnosis of Risk for Deficient Fluid Volume related to excessive fluid loss, secondary to diarrhea and vomiting was implemented for a home health client who began with these symptoms 5 days ago.
A goal was that the client's symptoms would be eliminated within 48 hours. The client is being seen after a week, and has had no diarrhea or vomiting for the past 5 days. The nurse should:
1. Keep the problem on the care plan, in case the symptoms return.
2. Document that the problem has been resolved and discontinue the care for the problem.
3. Assume that whatever the cause was, the symptoms may return, but document that the goal was met.
4. Document that the potential problem is being prevented since the symptoms have stopped.
Question 2
The written goal statement in a client's care plan is: Client will have clear lung sounds bilaterally within 3 days.
One of the interventions to meet this goal is that the nurse will teach the client to cough and deep breathe and have the client do this several times every 2 hours. At the end of the third day, the client's lungs are indeed clear. In order to relate the intervention to the outcome, the nurse should:
1. Ask how many times per day the client practiced the coughing and deep breathing exercises.
2. Tell the client that the lungs are clear.
3. Document the assessment findings to show the effectiveness of the intervention.
4. Write this evaluation statement: Goal met, lung sounds clear by third day.

 Mother zebra nursing her foal
Mother zebra nursing her foal
 Secondary intravenous lines: (a) a tandem intravenous alignment
Secondary intravenous lines: (a) a tandem intravenous alignment
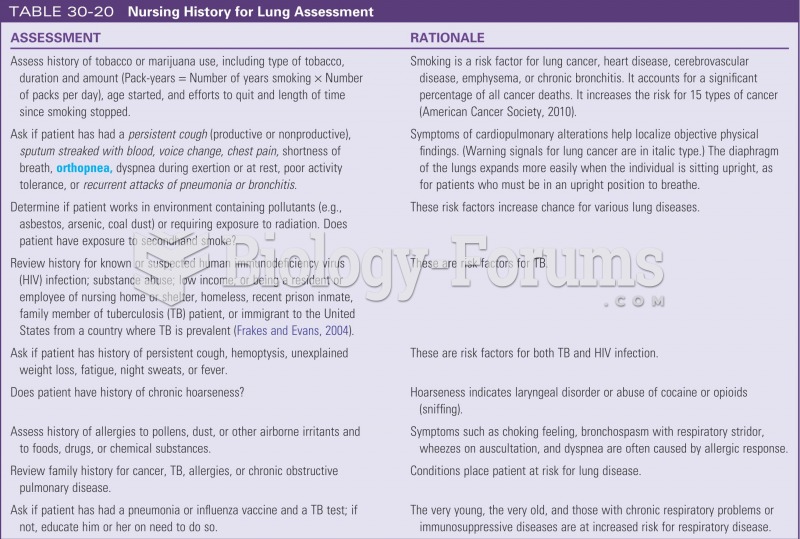 Nursing history for lung assessment
Nursing history for lung assessment
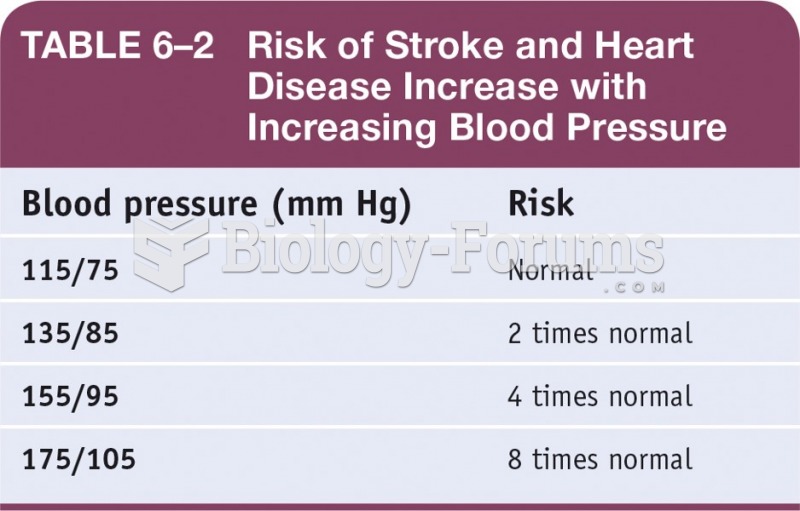 Risk of Stroke and Heart Disease Increase with Increasing Blood Pressure
Risk of Stroke and Heart Disease Increase with Increasing Blood Pressure
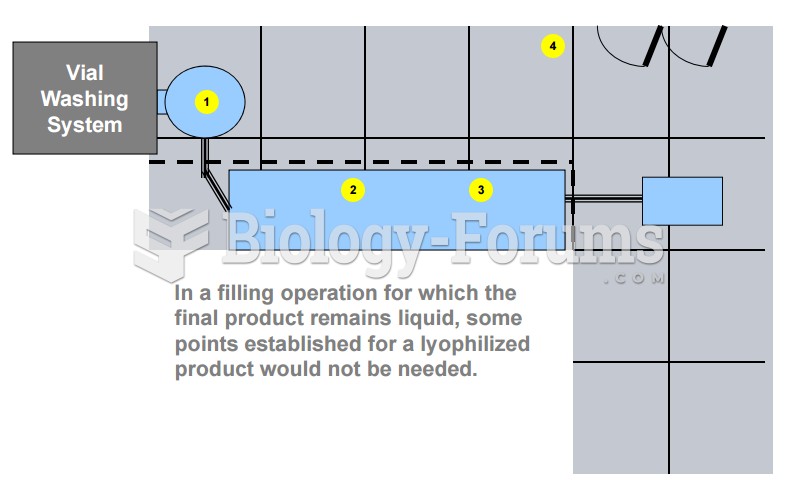 Vial Washing System - Risk Based Approach
Vial Washing System - Risk Based Approach
 Group defenses: Cluster of sawfly caterpillars regurgitating fluid (yellow) that predators find unap
Group defenses: Cluster of sawfly caterpillars regurgitating fluid (yellow) that predators find unap