Answer to Question 1
Correct Answer: 1
Rationale 1: The Minimum Data Set (MDS) for assessment and care screening must be performed within 4 days of a client's admission to a long-term care facility and reviewed every 3 months. Laws influencing the kind and frequency of documentation required are the Health Care Financing Administration and the Omnibus Budget Reconciliation Act (OBRA) of 1987.
Rationale 2: Laws influencing the kind and frequency of documentation required are the Health Care Financing Administration and the Omnibus Budget Reconciliation Act (OBRA) of 1987.
Rationale 3: CBE stands for charting by exception and is not the form of documentation used for this type of assessment.
Rationale 4: Kardex is a system of organizing client information so it can be accessed quickly. It is usually used in the acute care area.
Answer to Question 2
Correct Answer: 4
Rationale 1: The medical record contains this type of information, but the complete chart is lengthy and would take the student more time to review.
Rationale 2: The MAR includes only those medications that are prescribed or scheduled to be administered during the client's stay. It would not include other information like diagnostic tests, daily care, and so on.
Rationale 3: The written care plan may be utilized, but there is another more effective option available.
Rationale 4: The Kardex is a concise method of organizing and recording data about a client, making information quickly accessible to all health professionals. The system is on either an index-type file or a computer-generated form. Information is usually organized into sections: client history/information, list of medications, IV fluids, daily treatments and procedures, diagnostic procedures, allergies, how the client's physical needs are met (type of diet, bathing needs, etc.), and a problem list with stated goals.

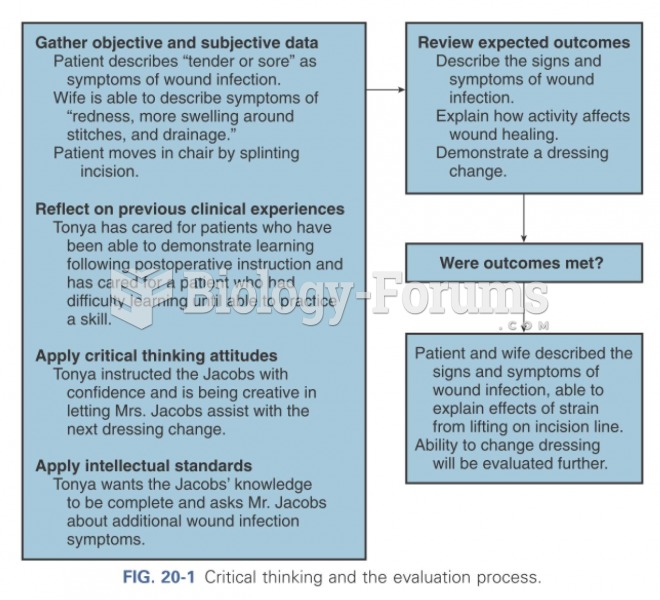 Critical thinking and the evaluation process
Critical thinking and the evaluation process
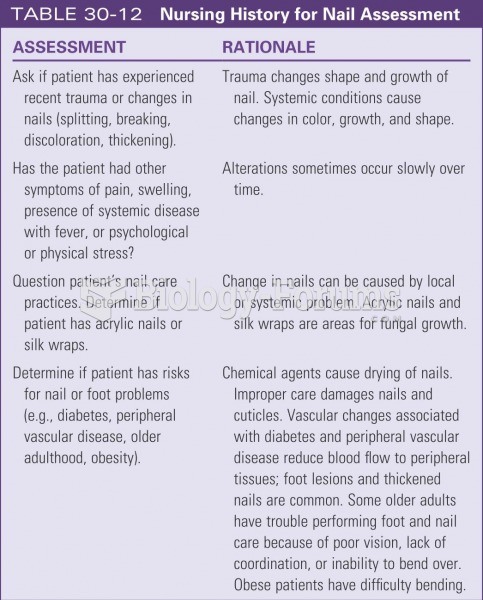 Nursing history for nail assessment
Nursing history for nail assessment
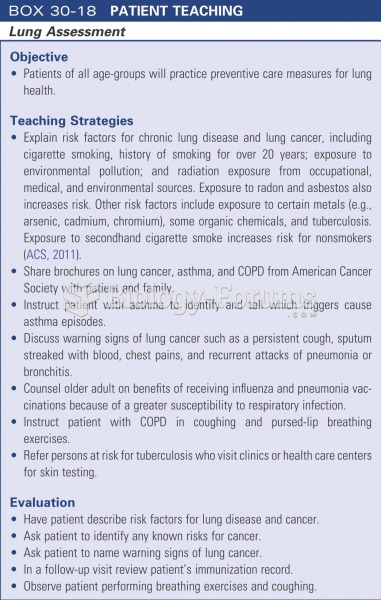 Patient teaching: lung assessment
Patient teaching: lung assessment
 Skilled nursing facilities provide care for patients requiring longer stays than hospitals allow.
Skilled nursing facilities provide care for patients requiring longer stays than hospitals allow.
 Take care
Take care
 Diagrammatic representation of the process of molecular hybridization
Diagrammatic representation of the process of molecular hybridization