Answer to Question 1
Correct Answer: 1, 2, 5
Rationale 1: Diagnosing is analyzing and synthesizing data in order to identify client strengths and health problems that can be prevented or resolved by collaborative and independent nursing interventions as well as developing a list of nursing and collaborative problems.
Rationale 2: Diagnosing is analyzing and synthesizing data in order to identify client strengths and health problems that can be prevented or resolved by collaborative and independent nursing interventions as well as developing a list of nursing and collaborative problems.
Rationale 3: Developing a plan is part of the planning phase.
Rationale 4: Specifying goals and outcomes is part of the planning phase.
Rationale 5: Diagnosing is analyzing and synthesizing data in order to identify client strengths and health problems that can be prevented or resolved by collaborative and independent nursing interventions as well as developing a list of nursing and collaborative problems.
Answer to Question 2
Correct Answer: 3
Rationale 1: Cues are subjective or objective data that can be directly observed by the nurse.
Rationale 2: Validation is the act of double-checking or verifying data to confirm that they are accurate and factual.
Rationale 3: Inferences are the nurse's interpretations of conclusions made based on the cues, which in this case would be the frequent visits to the emergency department and the client's injuries. Data must be based on cues, and the nurse must be careful not to jump to conclusions.
Rationale 4: Judgment is not part of validation.

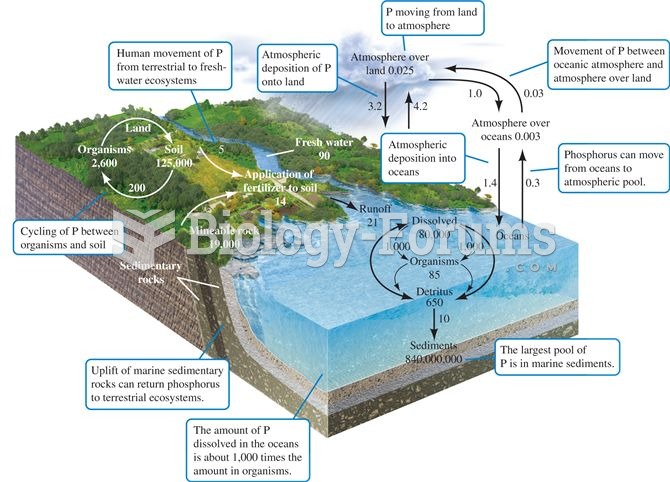 The phosphorus cycle. Numbers are 1012 g P or fluxes as 1012 g P per year (data from Schlesinger 199
The phosphorus cycle. Numbers are 1012 g P or fluxes as 1012 g P per year (data from Schlesinger 199
 When using an interpreter, the nurse should pose questions directly to the patient, not the interpre
When using an interpreter, the nurse should pose questions directly to the patient, not the interpre
 how a nursing student thinks
how a nursing student thinks
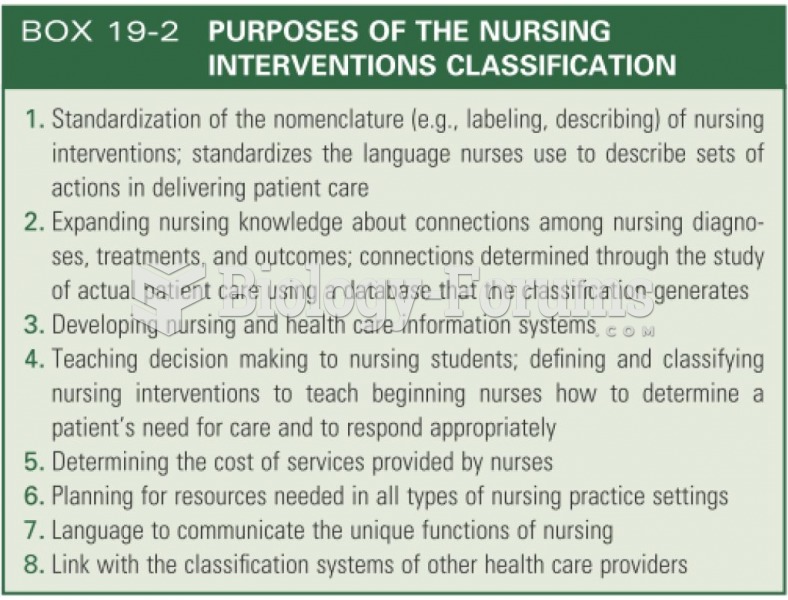 Purpose of the nursing interventions
Purpose of the nursing interventions
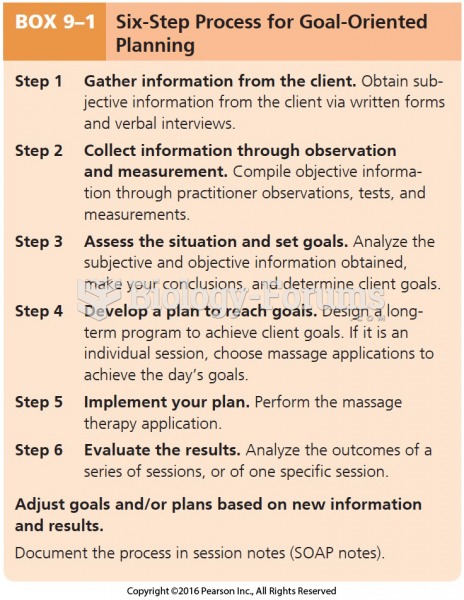 Six-Step Process for Goal-Oriented Planning
Six-Step Process for Goal-Oriented Planning
 Palpating the mastoid process
Palpating the mastoid process