Answer to Question 1
ANS: A
During the assessment step, patient care data are gathered through observation, interviews, and physical assessment. During the planning step of the nursing process, the nurse prioritizes the nursing diagnoses and identifies short- and long-term goals that are realistic, measurable, and patient focused, with specific outcome identification for evaluation purposes. The implementation step includes initiating specific nursing interventions and treatments designed to help the patient achieve established goals or outcomes. In the evaluation step, the nurse determines whether the patient's goals are met, examines the effectiveness of interventions, and decides whether the plan of care should be discontinued, continued, or revised.
Answer to Question 2
ANS: B
A two-part risk nursing diagnostic statement contains only (1) the patient's identified need or problem (i.e., NANDA-I nursing diagnostic label) and (2) factors indicating vulnerability (i.e., risk factors). The risk factor is the history of stroke. The chest discomfort and shortness of breath are symptoms of the current problems and would not be documented as potential or risk issues. Stroke would be the identified potential problem.

 A nurse prepares a client for anesthesia and surgery.
A nurse prepares a client for anesthesia and surgery.
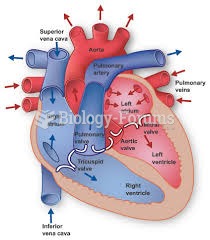 Anatomy of Heart
Anatomy of Heart
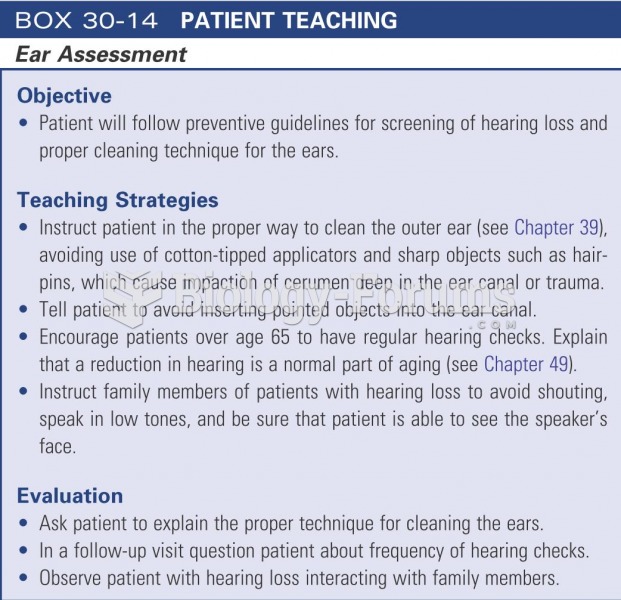 Patient teaching: ear assessment
Patient teaching: ear assessment
 A patient examination room should be simple and efficiently designed.
A patient examination room should be simple and efficiently designed.
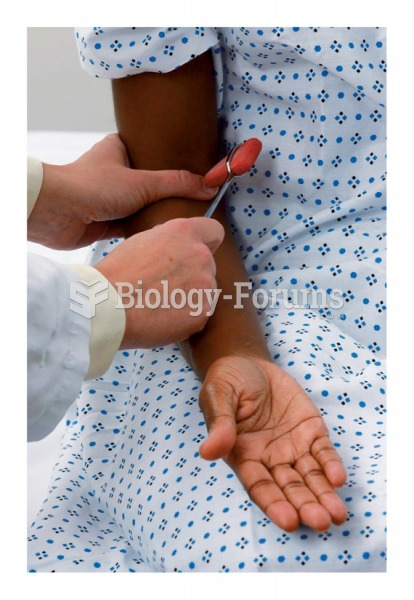 Testing the biceps reflex
Testing the biceps reflex
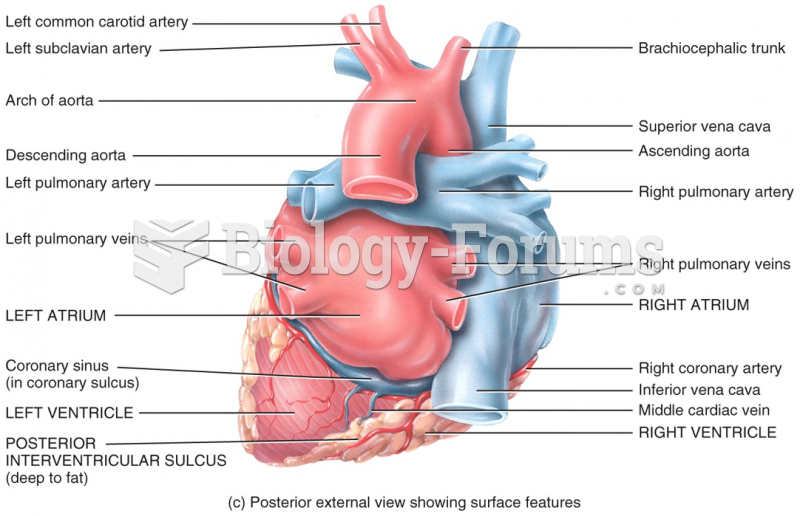 Chambers of the Heart
Chambers of the Heart