Answer to Question 1
ANS: A
There are three types of diagnoses: actual, risk, and health-promotion. Actual diagnoses have three parts: problem, etiology, and signs/symptoms. Risk diagnoses include only the identified need and the risk factors. The nursing diagnosis, imbalanced nutrition: less than body requirements, is missing the problem, etiology, and signs and symptoms. Impaired physical mobility is missing the evidence. Risk for suffocation should have only two parts. There are no signs and symptoms if the patient is at risk.
Answer to Question 2
ANS: A
All nursing interventions that are implemented for patients must be documented or charted. In some cases, this may involve checking off an intervention in the patient's EMR designed to track the effectiveness of specific interventions. Many health care agencies have special requirements for documenting interventions such as the use of physical restraints or pain protocols. Proper documentation of interventions facilitates communication with all members of the health care team and provides an essential legal record. Accurate charting helps to alleviate omissions and repetition of care. Documentation also allows nurses to evaluate the effectiveness of nursing interventions in meeting patient goals and outcomes, which is the final step in the nursing process.

 Tattoos and Body Piercings: This patient developed cellulitis from tattoo ink
Tattoos and Body Piercings: This patient developed cellulitis from tattoo ink
 An emergency medical technician positions defibrillator paddles on the chest of a supine male patien
An emergency medical technician positions defibrillator paddles on the chest of a supine male patien
 The medical assistant will provide patient education regarding the daily use of diabetic glucose ...
The medical assistant will provide patient education regarding the daily use of diabetic glucose ...
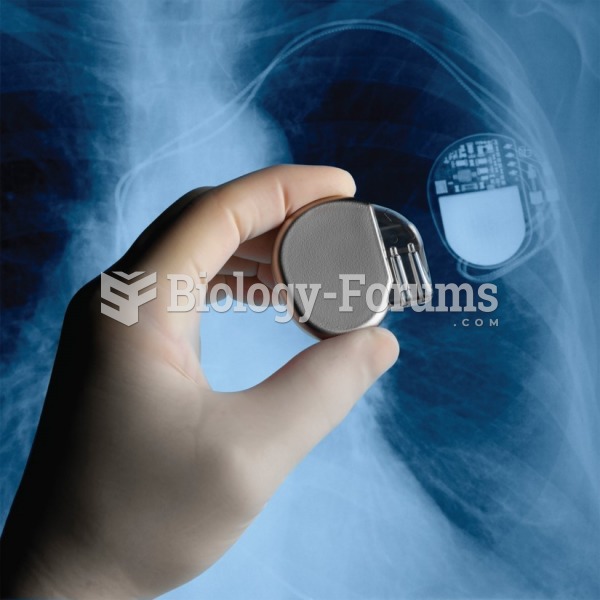 A surgeon holds a pacemaker next to an X-ray of a pacemaker implanted in a patient’s chest.
A surgeon holds a pacemaker next to an X-ray of a pacemaker implanted in a patient’s chest.
 Patient with DiGeorge syndrome. Note low set ears and wide set downward slanting eyes; often these ...
Patient with DiGeorge syndrome. Note low set ears and wide set downward slanting eyes; often these ...
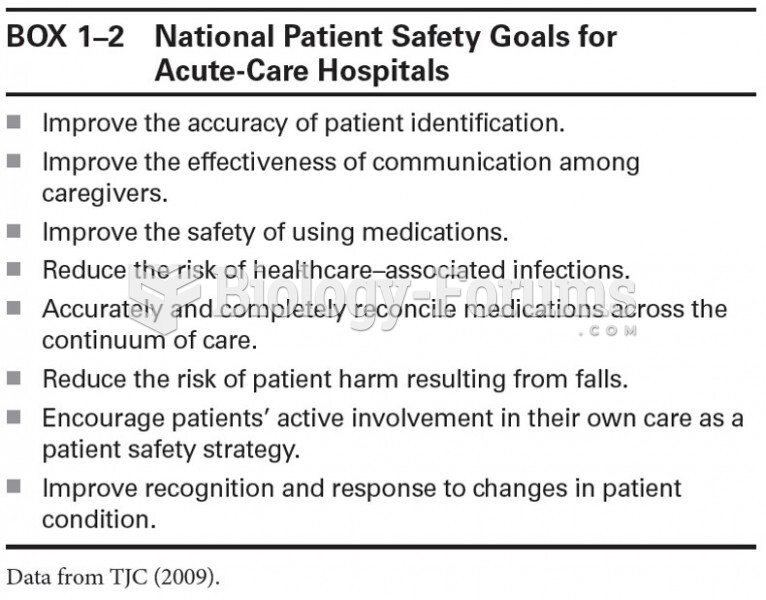 National Patient Safety Goals for Acute-Care Hospitals
National Patient Safety Goals for Acute-Care Hospitals