Answer to Question 1
ANS: A, B, C
CA-MRSA is thought to be present in 20 to 30 of the population, and many of these individuals are asymptomatic carriers. Boils caused by CA-MRSA can often be treated by surgical drainage alone. CA-MRSA is less dangerous than HA-MRSA but more dangerous than methicillin-sensitive Staphylococcus aureus (MSSA). CA-MRSA generally causes mild skin infections but can cause more serious infections, such as necrotizing fasciitis. CA-MRSA is transmitted by skin-to-skin contact and by contact with contaminated objects.
Answer to Question 2
ANS: C
Allergy to penicillin can decrease over time; therefore, in patients with a previous allergic reaction who need to take penicillin, skin tests can be performed to assess the current risk. Until this risk is known, changing to a cephalosporin is not necessary. Reassuring the patient that allergic responses will diminish is not correct, because this is not always the case; the occurrence of a reaction must be confirmed with skin tests. Desensitizing schedules are used when patients are known to be allergic and the drug is required anyway.

 Awareness of cultural and religious norms and customs will help you deliver appropriate nursing care
Awareness of cultural and religious norms and customs will help you deliver appropriate nursing care
 Nursing school
Nursing school
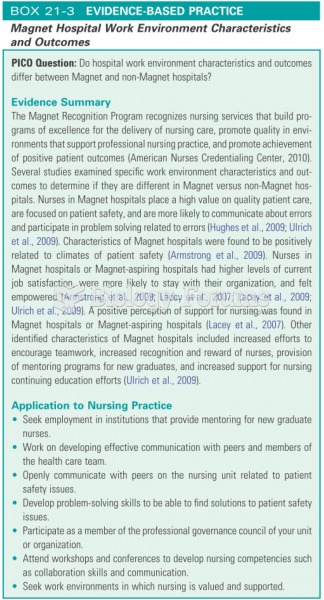 Magnet hospital nurse requirements
Magnet hospital nurse requirements
 How to use L’Hospital’s Rule to find the limit of a function (Part 3)
How to use L’Hospital’s Rule to find the limit of a function (Part 3)
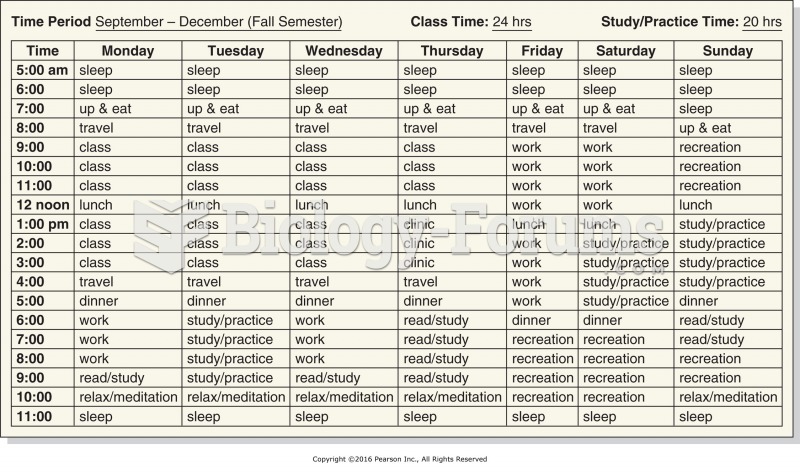 Sample time management planning chart for a massage student.
Sample time management planning chart for a massage student.
 Fundamental Concepts and Skills for Nursing
Fundamental Concepts and Skills for Nursing