Answer to Question 1
ANS: A, C, D
Treatment with beta blockers should continue at least 2 to 3 years and perhaps longer. Beta blockers have been found to reduce recurrent ischemia and reinfarction. Prolonged therapy with aspirin (81 to 162 mg/day) reduces the risk of reinfarction, stroke, and death. ACE inhibitor therapy should continue for 6 weeks in all patients with STEMI, barring contraindication, and indefinitely in patients with LV dysfunction.
Low-dose vitamin E and acetaminophen are not indicated in patients with STEMI.
Answer to Question 2
ANS: A
Aspirin suppresses platelet aggregation and produces an immediate antithrombotic effect, which is necessary for a patient who may be experiencing a myocardial infarction (MI). Although the patient is not experiencing chest pain, other, associated symptoms, as well as the history, could lead to suspicion of MI.
Aspirin does have analgesic properties. However, the question asks about the action of aspirin regarding the anginal equivalent (shortness of breath) and cardiac history. Aspirin is not going to decrease the shortness of breath but rather will assist with the antithrombotic effect.
Aspirin does not potentiate the effects of morphine. In addition, the patient has not received any morphine.
Aspirin has no vasodilatory properties.

 Nurse-patient interaction; nonverbal communication
Nurse-patient interaction; nonverbal communication
 Taking a Patient’s Oral Temperature with an Electronic Thermometer
Taking a Patient’s Oral Temperature with an Electronic Thermometer
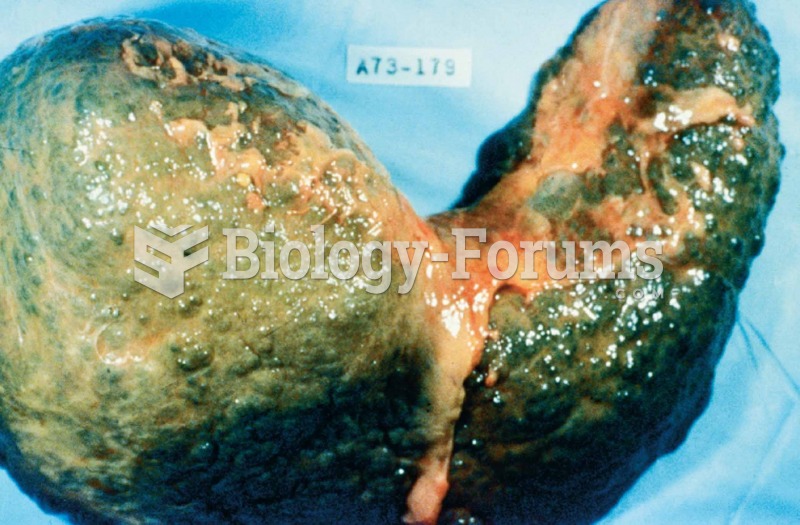 The liver in this photograph was from a deceased patient with an advanced state of cirrhosis.
The liver in this photograph was from a deceased patient with an advanced state of cirrhosis.
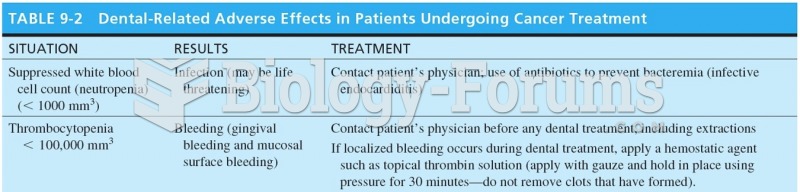 Dental Related Adverse Effects in Patients Undergoing Cancer Treatment
Dental Related Adverse Effects in Patients Undergoing Cancer Treatment