Answer to Question 1
Individual medications within the category of FDA-approved antidepressants typically reduce the symptoms in 50-60 of patientscompared with 20-30 response rate with placebo. However, some individuals who do not respond favorably to one type of antidepressant after adequate dosage and length of treatment may respond favorably to another in a different class, e.g., SSRIs, MAOIs, or another drug within the same class, or some combination of antidepressant medications. Tolerability of side effects of the particular antidepressant for the individual may dictate treatment compliance and efficacy.
Answer to Question 2
The actions and behavioral effects of reserpine, MAOIs, amphetamine, and monoamine reuptake blockers are superficially compatible with the hypothesis, because these either deplete or enhance synaptic catecholamine levels, and correspondingly induce or reduce symptoms of depression. However, the lack of correspondence between the onset of drug action and the drugs' clinical efficacy, i.e., the fact that MAOIs and many antidepressants enhance synaptic catecholamine levels rapidly (typically within hours) but exert their benefits in depressed individuals fairly slowly (typically within several days or weeks), is a problem for the hypothesis. Also, clinically effective catecholamine-augmenting antidepressants only elevate mood in depressed individuals. Also, the SSRIs, which have minimal influence on catecholamines, are just as effective as antidepressants as drugs that are potent catecholamine reuptake blockers.

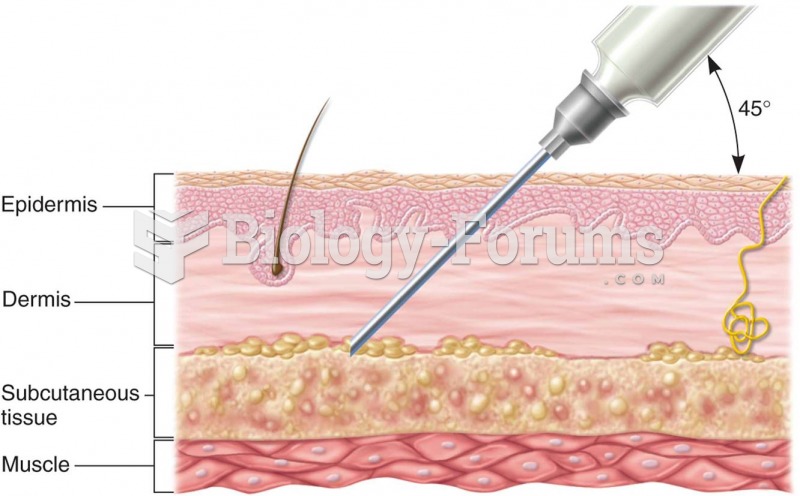 Subcutaneous drug administration: (a) cross section of skin showing depth of needle insertion;
Subcutaneous drug administration: (a) cross section of skin showing depth of needle insertion;
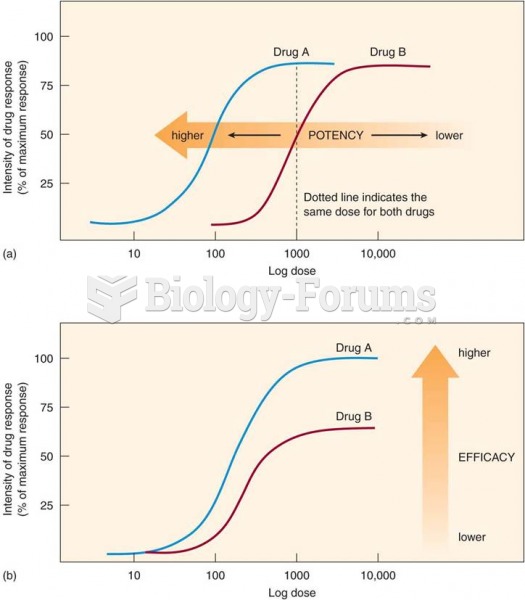 Potency and efficacy: (a) drug A has a higher potency than drug B; (b) drug A has a higher efficacy
Potency and efficacy: (a) drug A has a higher potency than drug B; (b) drug A has a higher efficacy
 Many older adults live active lives well into their eighties and beyond.
Many older adults live active lives well into their eighties and beyond.
 Hands-on class in a massage therapy program.
Hands-on class in a massage therapy program.
 A 2-kg box of taffy candy has 40 J of potential energy relative to the ground. Its height above ...
A 2-kg box of taffy candy has 40 J of potential energy relative to the ground. Its height above ...
 The current status of gene therapy worldwide
The current status of gene therapy worldwide