Answer to Question 1
Martin Seligman discovered that dogs and rats have an interesting emotional reaction to events over which they have no control. If rats receive occasional shocks, they can function reasonably well as long as they can cope with the shocks by doing something to avoid them, such as pressing a lever. But if they learn that nothing they do helps them avoid the shocks, they eventually become helpless, give up, and manifest an animal equivalent of depression. Seligman suggests we seem to do the same thing, but only under one important condition: people become anxious and depressed when they decide that they have no control over the stress in their lives. These findings evolved into an important model called the learned helplessness theory of depression. Often overlooked is Seligman's point that anxiety is the first response to a stressful situation. Depression may follow marked hopelessness about coping with the difficult life events. The depressive attributional style is (1) internal, in that the individual attributes negative events to personal failings (it is all my fault); (2) stable, in that, even after a particular negative event passes, the attribution that additional bad things will always be my fault remains; and (3) global, in that the attributions extend across a variety of issues.
An example of an upsetting event is being placed in a nursing home. In a relatively short amount of time, the patient realizes that he/she has lost all control over his/her life, becoming stressed as every decision is made for him/her by family, caregivers, and personnel. The patient feels anxious, afraid, and eventually depressed. Often the feelings of helplessness turn to hopelessness and the person gives up.
Answer to Question 2
In family studies, when you look at the prevalence of a given disorder in the first-degree relatives of an individual known to have the disorder (the proband), despite wide variability, the rate in relatives of probands with mood disorders is consistently about two to three times greater than in relatives of controls who don't have mood disorders. The best evidence that genes have something to do with mood disorders comes from twin studies. If a genetic contribution exists, the disorder should be present in identical twins to a much greater extent than in fraternal twins. An identical twin is two to three times more likely to present with a mood disorder than a fraternal twin if the first twin has a mood disorder.
Research implicates low levels of serotonin in the causes of mood disorders, but only in relation to other neurotransmitters, including norepinephrine and dopamine. The apparent primary function of serotonin is to regulate our emotional reactions. For example, we are more impulsive, and our moods swing more widely, when our levels of serotonin are low. This may be because one of the functions of serotonin is to regulate systems involving norepinephrine and dopamine. According to the permissive hypothesis, when serotonin levels are low, other neurotransmitters are permitted to range more widely, become dysregulated, and contribute to mood irregularities, including depression. A drop in norepinephrine would be one of the consequences. Current thinking is that the balance of the various neurotransmitters and their interaction with systems of self-regulation are more important than the absolute level of any one neurotransmitter.

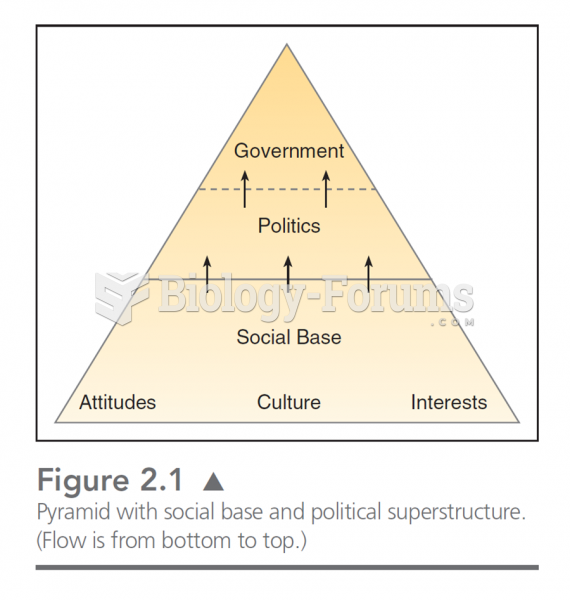 This chart illustrates the bottom up assumption about government. In this, attitudes, culture, and
This chart illustrates the bottom up assumption about government. In this, attitudes, culture, and
 Contact theory indicates that prejudice decreases and relations improve when individuals of ...
Contact theory indicates that prejudice decreases and relations improve when individuals of ...
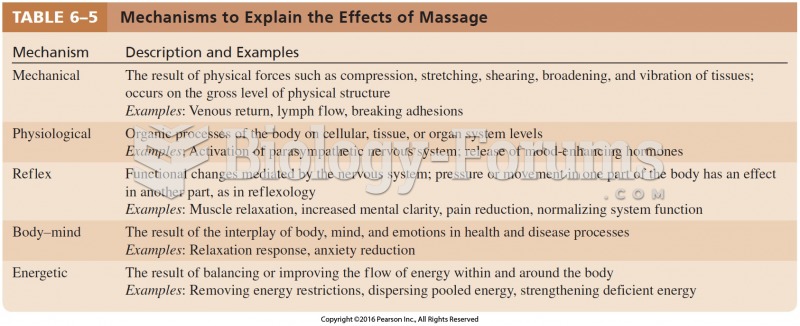 Mechanisms to Explain the Effects of Massage
Mechanisms to Explain the Effects of Massage
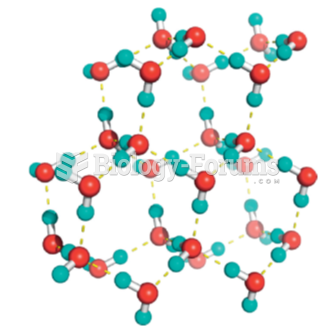 A skeletal model of the ice lattice
A skeletal model of the ice lattice
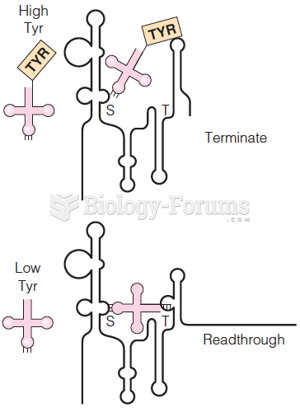 Model for induction of B. subtilis tyrS gene by uncharged tRNATyr
Model for induction of B. subtilis tyrS gene by uncharged tRNATyr
 Holley’s two-dimensional cloverleaf model of transfer RNA
Holley’s two-dimensional cloverleaf model of transfer RNA